The Child Care and Development Fund (CCDF) is a federally-funded program that helps states improve their child care systems. CCDF funds can be used for a variety of purposes, including helping families afford quality child care, improving the quality of care in licensed or regulated programs, and increasing the availability of affordable high-quality child care. Every state has its own CCDF program, so be sure to contact your state's department of early childhood development or human services to learn more about how to apply. This blog post will provide an overview of CCDF and explain how to access these funds if you are a parent or provider. Stay tuned for future posts that will go into more detail about each type of funding available through CCDF.
| Question | Answer |
|---|---|
| Form Name | Ccdf Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ccdf form printable, ccdf discrepancy, ccdf form download, how to ccdf form |
|
|
|
|
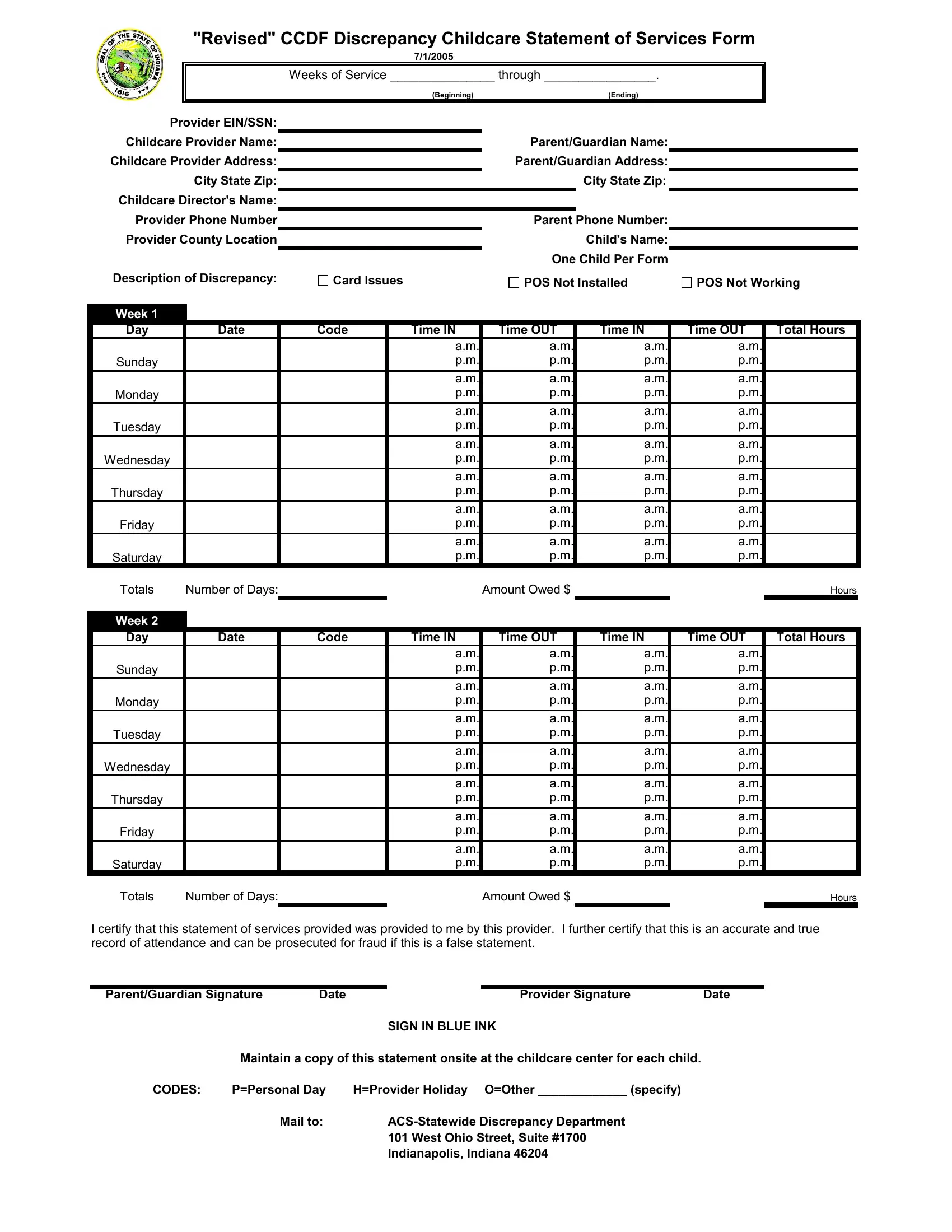
"Revised" CCDF Discrepancy Childcare Statement of Services Form |
|
||||||||||||
|
|
|
|
|
|
|
|
|
7/1/2005 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weeks of Service _______________ through ________________. |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
(Beginning) |
|
|
|
(Ending) |
|
|
|
|
|
|
|
Provider EIN/SSN: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Childcare Provider Name: |
|
|
|
|
|
|
|
Parent/Guardian Name: |
|
|
|
|
|||
|
|
Childcare Provider Address: |
|
|
|
|
|
|
Parent/Guardian Address: |
|
|
|
|
||||
|
|
|
|
City State Zip: |
|
|
|
|
|
|
|
|
City State Zip: |
|
|
|
|
|
|
Childcare Director's Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Provider Phone Number |
|
|
|
|
|
|
|
Parent Phone Number: |
|
|
|
|
|||
|
|
Provider County Location |
|
|
|
|
|
|
|
|
Child's Name: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
One Child Per Form |
|
|
|
|
|
|
|
Description of Discrepancy: |
|
|
Card Issues |
|
|
|
POS Not Installed |
|
|
POS Not Working |
|||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Week 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Day |
|
Date |
Code |
|
Time IN |
Time OUT |
Time IN |
|
Time OUT |
Total Hours |
|||||
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Sunday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Monday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Tuesday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Wednesday |
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Thursday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Friday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
a.m. |
|
|
a.m. |
a.m. |
|
|
a.m. |
|
|
|
Saturday |
|
|
|
|
|
|
p.m. |
|
|
p.m. |
p.m. |
|
|
p.m. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Totals |
Number of Days: |
|
|
Amount Owed $ |
|
|
Hours |
Week 2 |
|
|
|
|
|
|
|
Day |
Date |
Code |
Time IN |
Time OUT |
Time IN |
Time OUT |
Total Hours |
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Sunday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Monday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Tuesday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Wednesday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Thursday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Friday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
|
|
|
a.m. |
a.m. |
a.m. |
a.m. |
|
Saturday |
|
|
p.m. |
p.m. |
p.m. |
p.m. |
|
Totals |
Number of Days: |
|
|
Amount Owed $ |
|
|
Hours |
I certify that this statement of services provided was provided to me by this provider. I further certify that this is an accurate and true record of attendance and can be prosecuted for fraud if this is a false statement.
Parent/Guardian Signature |
Date |
|
Provider Signature |
Date |
SIGN IN BLUE INK
Maintain a copy of this statement onsite at the childcare center for each child.
CODES: |
P=Personal Day |
H=Provider Holiday O=Other _____________ (specify) |
|
Mail to: |
|
|
|
101 West Ohio Street, Suite #1700 |
|
|
Indianapolis, Indiana 46204 |