
scaffold request form pdf can be completed effortlessly. Just make use of FormsPal PDF tool to do the job promptly. We are focused on providing you the perfect experience with our editor by regularly presenting new capabilities and improvements. With these improvements, using our tool becomes easier than ever before! It just takes just a few simple steps:
Step 1: Open the PDF in our editor by pressing the "Get Form Button" in the top section of this webpage.
Step 2: The editor allows you to modify your PDF document in a range of ways. Change it with personalized text, adjust what's already in the file, and place in a signature - all close at hand!
Concentrate while filling out this pdf. Ensure every single blank field is filled out correctly.
1. While filling in the scaffold request form pdf, be certain to include all needed blanks in their associated form section. It will help to speed up the process, making it possible for your information to be processed efficiently and correctly.

2. Soon after the prior section is done, go on to enter the applicable details in these - Request for, DME, Supplies, Private Duty Nursing, PPECC, Inpatient Rehabilitation, Other, A Client Information, Client Name Last First MI, Medicaid Number, Date of Birth, B Rendering, Name, Street Address, and City.
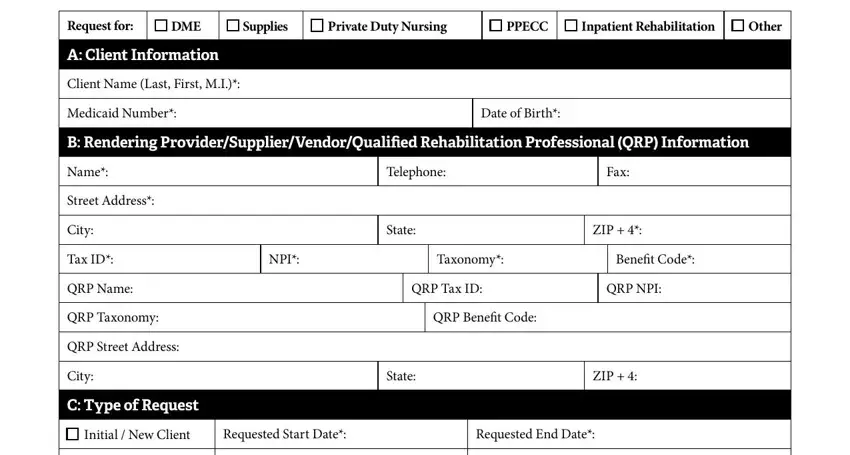
In terms of DME and City, ensure you double-check them in this section. These are viewed as the most significant ones in the PDF.
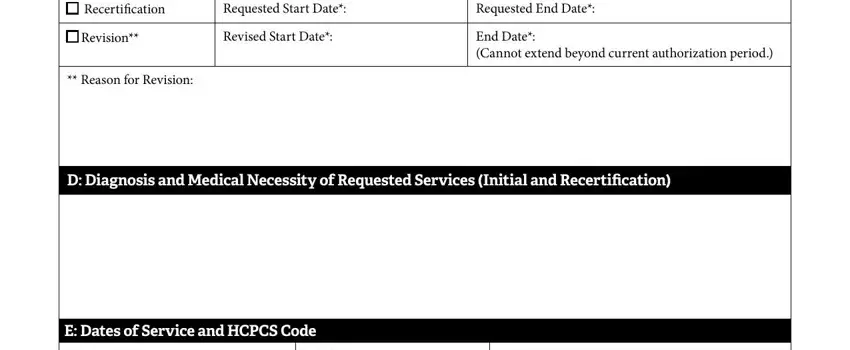
3. This next part is focused on Recertification, Requested Start Date, Requested End Date, Revision, Revised Start Date, End Date Cannot extend beyond, Reason for Revision, D Diagnosis and Medical Necessity, and E Dates of Service and HCPCS Code - fill in these empty form fields.
4. To go onward, this fourth part involves typing in a few empty form fields. These include HCPCS Code Modifier, Brief Description of Requested, Quantity Frequency, Retail Price, EssentialCritical field, Page of, and Revised Effective, which you'll find key to going forward with this form.

5. Lastly, the following last segment is precisely what you will have to wrap up prior to finalizing the document. The fields in question are the following: E Dates of Service and HCPCS Code, Note HCPCS codes and descriptions, F Primary Practitioners, By requesting the identified DME, The client is under years of age, By requesting Private Duty Nursing, and The client is under years of age.
Step 3: Prior to moving forward, double-check that all blank fields have been filled out the proper way. The moment you establish that it's fine, click on “Done." After getting a7-day free trial account at FormsPal, it will be possible to download scaffold request form pdf or send it via email at once. The document will also be readily available via your personal account page with your each and every change. We do not share or sell any details that you use while dealing with forms at FormsPal.