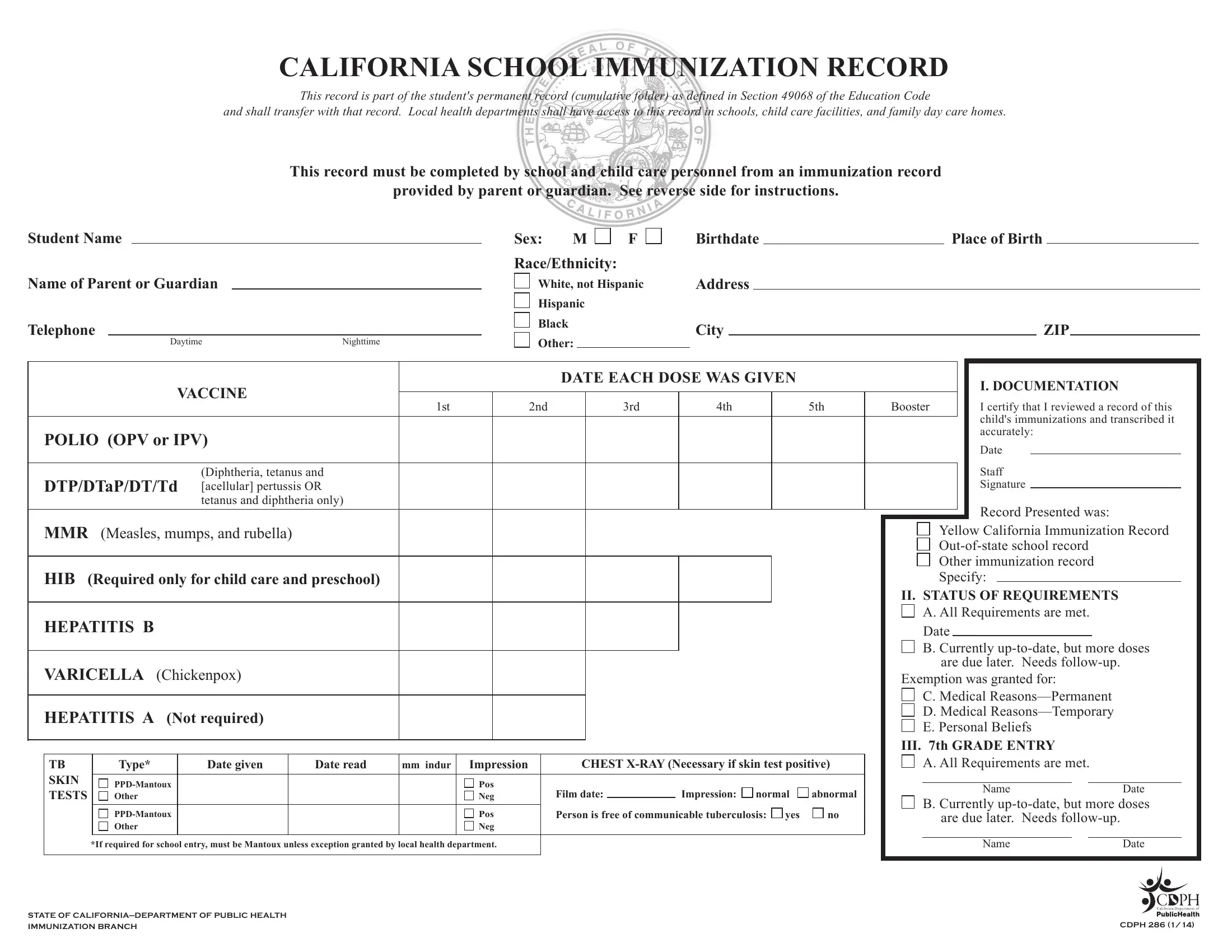
The California School Immunization Record (CDPH 286) is a mandatory document for students enrolling in California schools, child care facilities, and family day care homes. It is part of the student's permanent cumulative folder as defined under Education Code Section 49068, documenting each student's immunization status to support school enrollment compliance statewide.
The CDPH 286 form is required for children entering California public or private schools, licensed child care facilities, and family day care homes. Any student transferring between California schools must also have an updated immunization record on file. School or childcare personnel complete the form based on an immunization record provided by the parent or guardian.
The CDPH 286 immunization record documents the student's name, birthdate, and place of birth, along with a detailed vaccination history showing vaccine types, dates administered, and required follow-up doses. It includes sections for tuberculosis (TB) skin tests and chest X-ray results required in specific California jurisdictions. The reverse side provides comprehensive staff instructions for accurate completion of the record.
Students may qualify for medical exemptions documented by a licensed physician. Personal belief exemptions are recorded on the form with a required signature. The CDPH 286 form ensures schools verify compliance with California's immunization requirements for every enrolled student, supporting public health initiatives in educational settings across the state.
| Question | Answer |
|---|---|
| Form Name | CDPH 286 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 74 |
| Avg. time to fill out | 15 min 22 sec |
| Other names | california 286 school immunization record, blue immunization card, school immunization record, california immunization record printable |