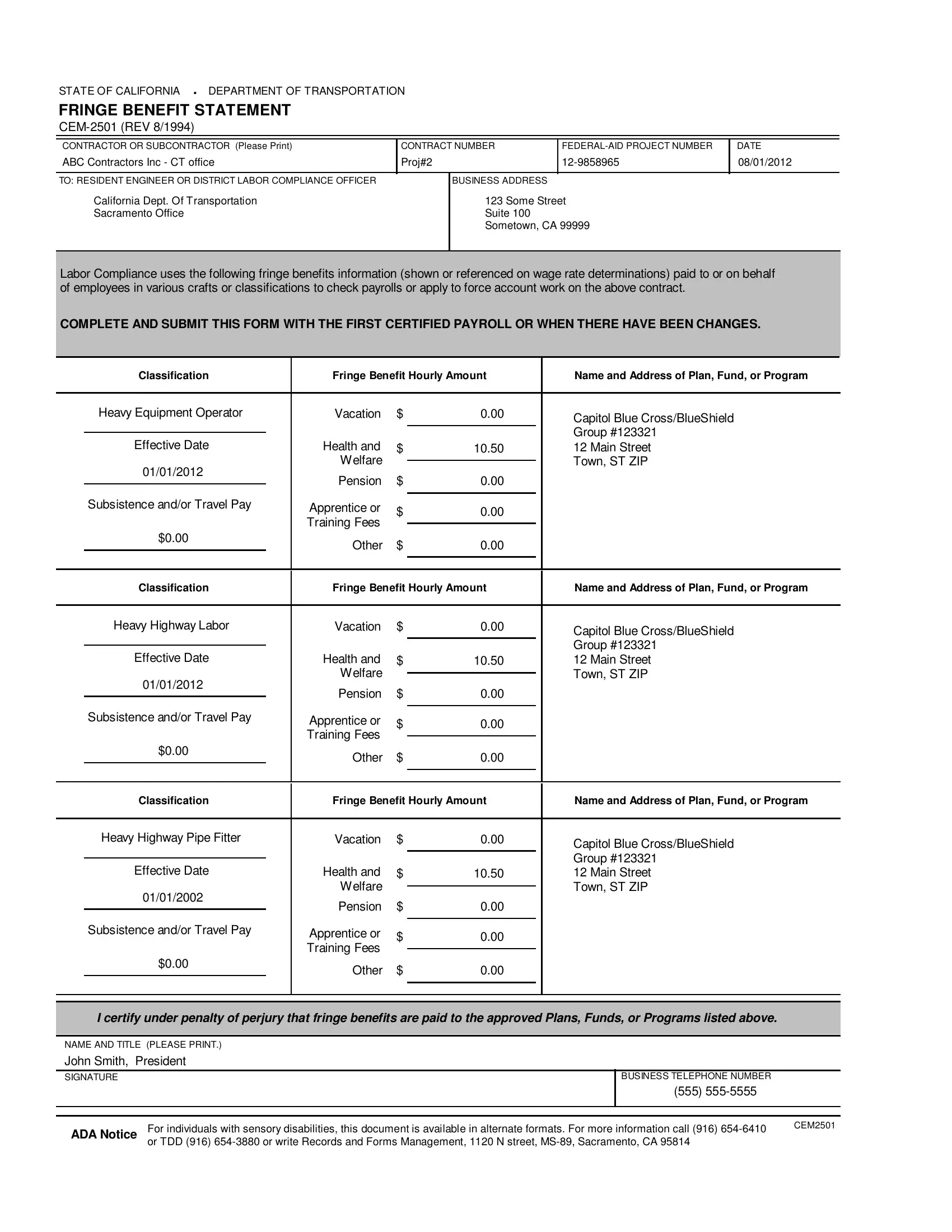
The State of California's Department of Transportation mandates the use of the Fringe Benefit Statement, known as CEM-2501, a crucial document for contractors or subcontractors engaged in federal-aid projects. This form serves as a transparent record, detailing the fringe benefits provided to employees across various classifications or crafts, such as health and welfare, pension, vacation, subsistence, travel pay, and apprenticeship or training fees. Contractors are required to accurately fill out and submit this form with their first certified payroll or upon any changes in fringe benefits, ensuring compliance with labor regulations. Each entry lists the type of benefit, the hourly amount, and the details of the plan, fund, or program providing the benefit, thereby enabling labor compliance officers or resident engineers to verify and apply these benefits to payroll checks or force account work connected to the specified contract. The form underscores the contractor's commitment to upholding the welfare of their workforce by detailing the benefits provided, reinforcing the importance of compliance and transparency in the allocation of fringe benefits to employees. This detailed documentation also caters to individuals with sensory disabilities, offering alternate formats upon request, underscoring the commitment to accessibility and inclusivity within the framework of labor compliance and contractor responsibilities.
| Question | Answer |
|---|---|
| Form Name | Cem 2501 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | california cem 2501, state of california cem 2501, cem 2501 fringe benefit statement, cem 2501 fillable |

STATE OF CALIFORNIA · DEPARTMENT OF TRANSPORTATION
FRINGE BENEFIT STATEMENT
CONTRACTOR OR SUBCONTRACTOR (Please Print) |
CONTRACT NUMBER |
DATE |
||
ABC Contractors Inc - CT office |
Proj#2 |
08/01/2012 |
||
|
|
|
|
|
TO: RESIDENT ENGINEER OR DISTRICT LABOR COMPLIANCE OFFICER |
|
BUSINESS ADDRESS |
|
|
California Dept. Of Transportation |
|
123 Some Street |
|
|
Sacramento Office |
|
Suite 100 |
|
|
|
|
Sometown, CA 99999 |
|
|
|
|
|
|
|
Labor Compliance uses the following fringe benefits information (shown or referenced on wage rate determinations) paid to or on behalf of employees in various crafts or classifications to check payrolls or apply to force account work on the above contract.
COMPLETE AND SUBMIT THIS FORM WITH THE FIRST CERTIFIED PAYROLL OR WHEN THERE HAVE BEEN CHANGES.
|
Classification |
Fringe Benefit Hourly Amount |
Name and Address of Plan, Fund, or Program |
|||||
|
|
|
|
|
|
|
|
|
|
Heavy Equipment Operator |
Vacation |
$ |
0.00 |
|
Capitol Blue Cross/BlueShield |
||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Group #123321 |
|
|
Effective Date |
Health and |
|
|
|
|||
|
$ |
10.50 |
|
12 Main Street |
||||
01/01/2012 |
|
Welfare |
|
|
|
Town, ST ZIP |
||
|
|
0.00 |
|
|||||
|
Pension |
$ |
|
|
|
|||
|
|
|
|
|
|
|||
|
Subsistence and/or Travel Pay |
|
|
|||||
|
Apprentice or |
$ |
|
|
|
|
||
|
0.00 |
|
|
|
||||
|
|
|
|
|
|
|||
|
|
|
Training Fees |
|
|
|
||
$0.00 |
|
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
Other |
$ |
0.00 |
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Classification |
Fringe Benefit Hourly Amount |
Name and Address of Plan, Fund, or Program |
|||||
|
|
|
|
|
|
|
|
|
|
Heavy Highway Labor |
Vacation |
$ |
0.00 |
|
Capitol Blue Cross/BlueShield |
||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Group #123321 |
|
|
Effective Date |
Health and |
|
|
|
|||
|
$ |
10.50 |
|
12 Main Street |
||||
01/01/2012 |
|
Welfare |
|
|
|
Town, ST ZIP |
||
|
|
0.00 |
|
|||||
|
Pension |
$ |
|
|
|
|||
|
|
|
|
|
|
|||
|
Subsistence and/or Travel Pay |
|
|
|
||||
|
Apprentice or |
$ |
|
|
|
|
||
|
0.00 |
|
|
|
||||
|
|
|
|
|
|
|||
|
|
|
Training Fees |
|
|
|
||
$0.00 |
|
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
Other |
$ |
0.00 |
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Classification |
Fringe Benefit Hourly Amount |
Name and Address of Plan, Fund, or Program |
|||||
|
|
|
|
|
|
|
|
|
|
Heavy Highway Pipe Fitter |
Vacation |
$ |
0.00 |
|
Capitol Blue Cross/BlueShield |
||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Group #123321 |
|
|
Effective Date |
Health and |
|
|
|
|||
|
$ |
10.50 |
|
12 Main Street |
||||
01/01/2002 |
|
Welfare |
|
|
|
Town, ST ZIP |
||
|
|
|
|
|||||
|
Pension |
$ |
0.00 |
|
|
|
||
|
|
|
|
|
|
|||
|
Subsistence and/or Travel Pay |
|
|
|
||||
|
Apprentice or |
|
|
|
|
|
||
|
$ |
0.00 |
|
|
|
|||
|
|
|
|
|
|
|||
|
|
|
Training Fees |
|
|
|
||
$0.00 |
|
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
Other |
$ |
0.00 |
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
I certify under penalty of perjury that fringe benefits are paid to the approved Plans, Funds, or Programs listed above. |
|||||||
|
|
|
|
|
|
|
||
NAME AND TITLE (PLEASE PRINT.) |
|
|
|
|
|
|
||
John Smith, President |
|
|
|
|
|
|
||
SIGNATURE |
|
|
|
|
|
BUSINESS TELEPHONE NUMBER |
||
|
|
|
|
|
|
|
|
(555) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADA Notice |
For individuals with sensory disabilities, this document is available in alternate formats. For more information call (916) |
CEM2501 |
|
||
or TDD (916) |
|
|
|
|