To Mail this request:
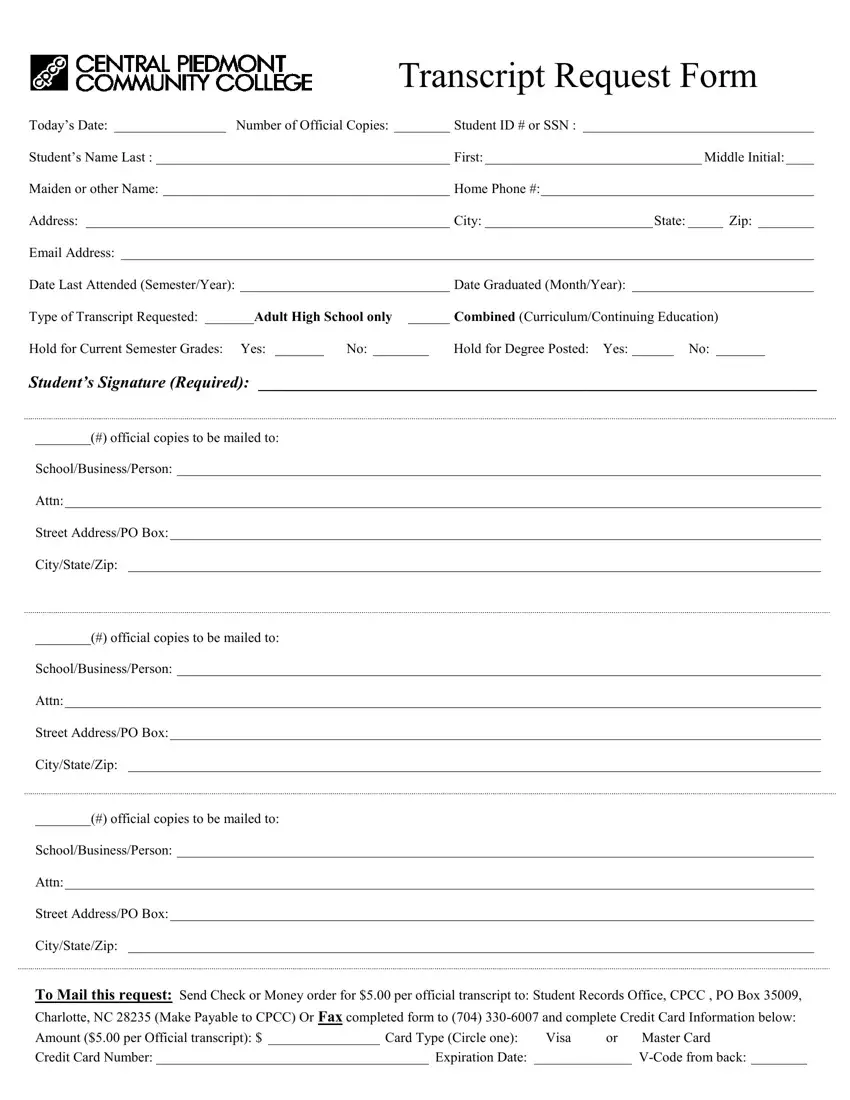
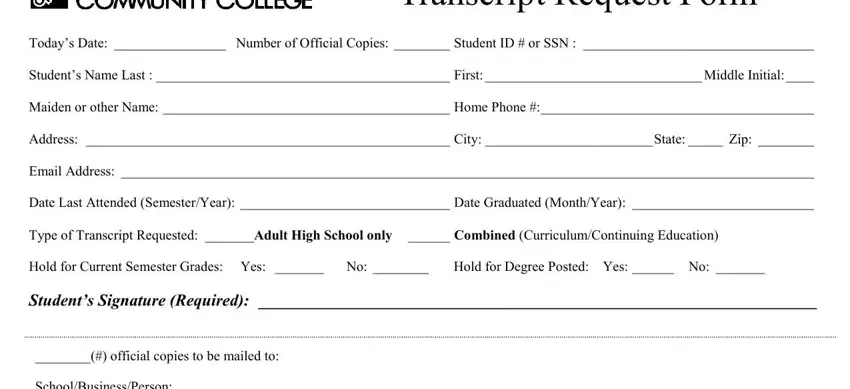
Transcript Request Form
Today’s Date: ________________ Number of Official Copies: ________ Student ID # or SSN : _________________________________
Student’s Name Last : __________________________________________ First:_______________________________ Middle Initial:____
Maiden or other Name: _________________________________________ Home Phone #:_______________________________________
Address: ____________________________________________________ City: ________________________State: _____ Zip: ________
Email Address: ___________________________________________________________________________________________________
Date Last Attended (Semester/Year): ______________________________ Date Graduated (Month/Year): __________________________
Type of Transcript Requested: _______Adult High School only ______ Combined (Curriculum/Continuing Education)
Hold for Current Semester Grades: Yes: _______ No: ________ Hold for Degree Posted: Yes: ______ No: _______
Student’s Signature (Required): ___________________________________________________________________
________(#) official copies to be mailed to:
School/Business/Person: ____________________________________________________________________________________________
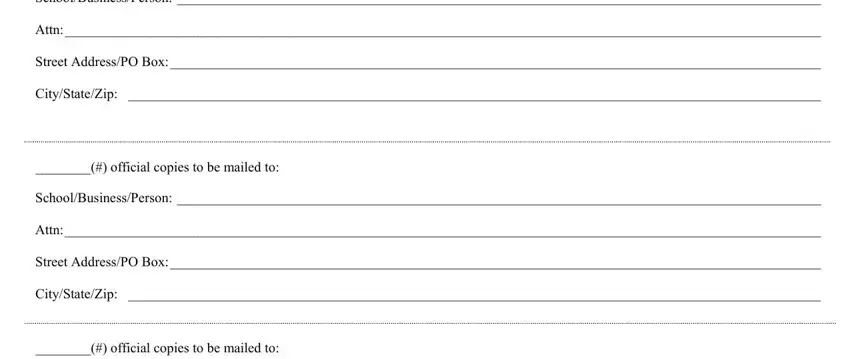
Attn:____________________________________________________________________________________________________________
Street Address/PO Box:_____________________________________________________________________________________________
City/State/Zip: ___________________________________________________________________________________________________
________(#) official copies to be mailed to:
School/Business/Person: ____________________________________________________________________________________________
Attn:____________________________________________________________________________________________________________
Street Address/PO Box:_____________________________________________________________________________________________
City/State/Zip: ___________________________________________________________________________________________________
________(#) official copies to be mailed to:
School/Business/Person: ___________________________________________________________________________________________
Attn:___________________________________________________________________________________________________________
Street Address/PO Box:____________________________________________________________________________________________
City/State/Zip: __________________________________________________________________________________________________
Send Check or Money order for $5.00 per official transcript to: Student Records Office, CPCC , PO Box 35009,
Charlotte, NC 28235 (Make Payable to CPCC) Or Fax completed form to (704) 330-6007 and complete Credit Card Information below:
Amount ($5.00 per Official transcript): $ ________________ Card Type (Circle one): Visa or Master Card
Credit Card Number: _______________________________________ Expiration Date: ______________ V-Code from back: ________