
With the help of the online PDF editor by FormsPal, you can fill out or edit where certificate death form download right here and now. To keep our tool on the leading edge of efficiency, we aim to integrate user-driven features and improvements regularly. We are always grateful for any feedback - play a pivotal part in revampimg PDF editing. Starting is effortless! All you need to do is adhere to the next simple steps down below:
Step 1: Firstly, access the tool by pressing the "Get Form Button" in the top section of this webpage.
Step 2: With this state-of-the-art PDF editor, you could do more than simply fill in blanks. Edit away and make your docs look great with customized textual content put in, or adjust the file's original content to excellence - all supported by the capability to incorporate your personal pictures and sign the file off.
This PDF doc will need some specific information; to ensure accuracy, you need to adhere to the next suggestions:
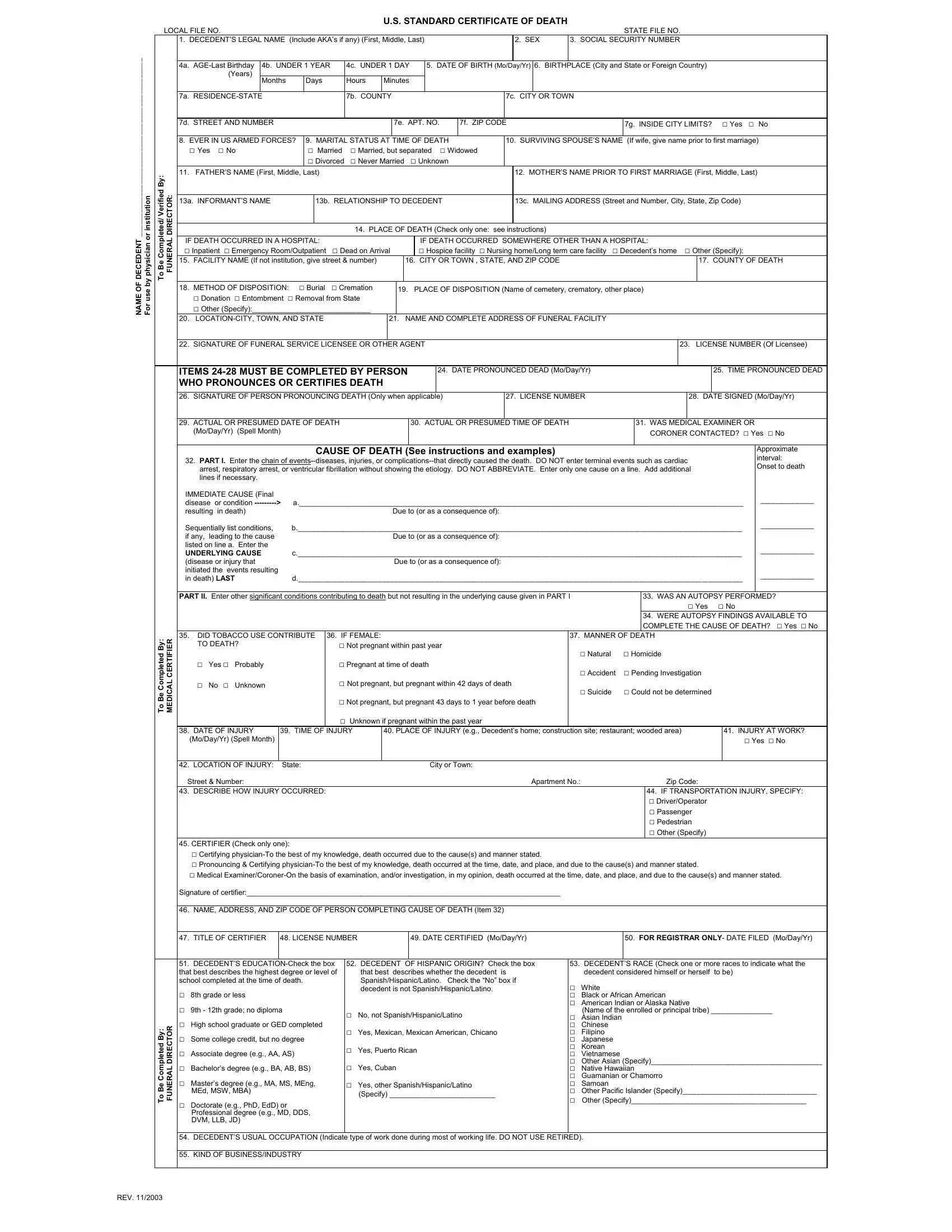
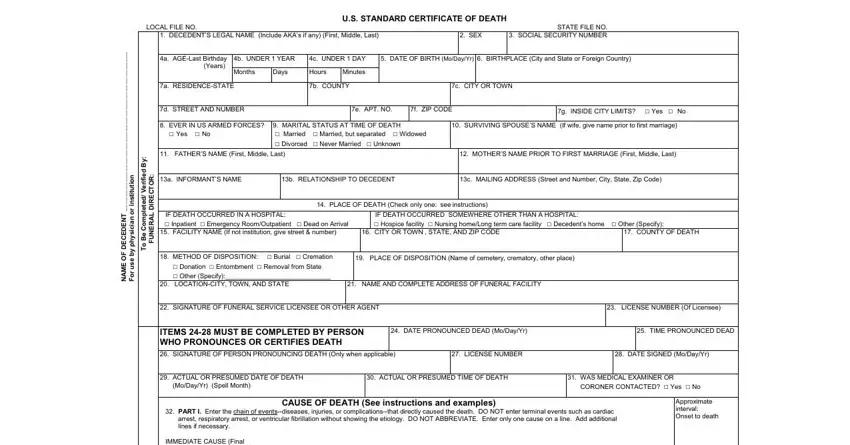
1. It's essential to fill out the where certificate death form download correctly, therefore be careful while filling in the sections including all these fields:
2. The next step is usually to submit the next few blanks: y B d e t e p m o C e B o T, R E F T R E C L A C D E M, IMMEDIATE CAUSE Final disease or, Sequentially list conditions b if, UNDERLYING CAUSE c, disease or injury that Due to or, PART II Enter other significant, WAS AN AUTOPSY PERFORMED cid Yes, DID TOBACCO USE CONTRIBUTE TO, IF FEMALE, cid Not pregnant within past year, cid Yes cid Probably, cid No cid Unknown, cid Pregnant at time of death, and cid Not pregnant but pregnant.
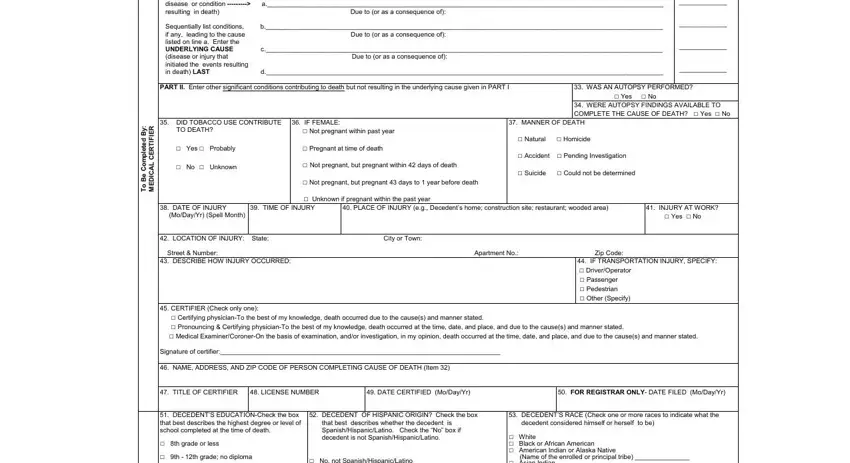
3. The following segment will be focused on y B d e t e l p m o C e B o T, R O T C E R D L A R E N U F, REV, DECEDENTS EDUCATIONCheck the box, cid No not SpanishHispanicLatino, DECEDENTS RACE Check one or more, DECEDENTS USUAL OCCUPATION, and KIND OF BUSINESSINDUSTRY - fill out each of these blanks.
Always be really mindful when filling in cid No not SpanishHispanicLatino and REV, as this is where a lot of people make a few mistakes.
Step 3: Check that the information is correct and simply click "Done" to conclude the project. Obtain your where certificate death form download as soon as you subscribe to a free trial. Easily access the pdf form from your personal cabinet, with any edits and changes being automatically saved! FormsPal offers safe document completion without data record-keeping or distributing. Be assured that your information is in good hands here!