
il background check form can be completed without any problem. Just make use of FormsPal PDF editor to perform the job fast. In order to make our editor better and simpler to use, we constantly come up with new features, with our users' feedback in mind. Starting is effortless! Everything you should do is follow the next easy steps down below:
Step 1: First, access the editor by pressing the "Get Form Button" at the top of this page.
Step 2: As soon as you access the PDF editor, you will find the form all set to be filled in. In addition to filling out different blanks, you could also do other things with the file, including writing your own textual content, modifying the initial textual content, inserting images, placing your signature to the form, and a lot more.
This document will need specific details; in order to guarantee accuracy and reliability, remember to take heed of the recommendations further down:
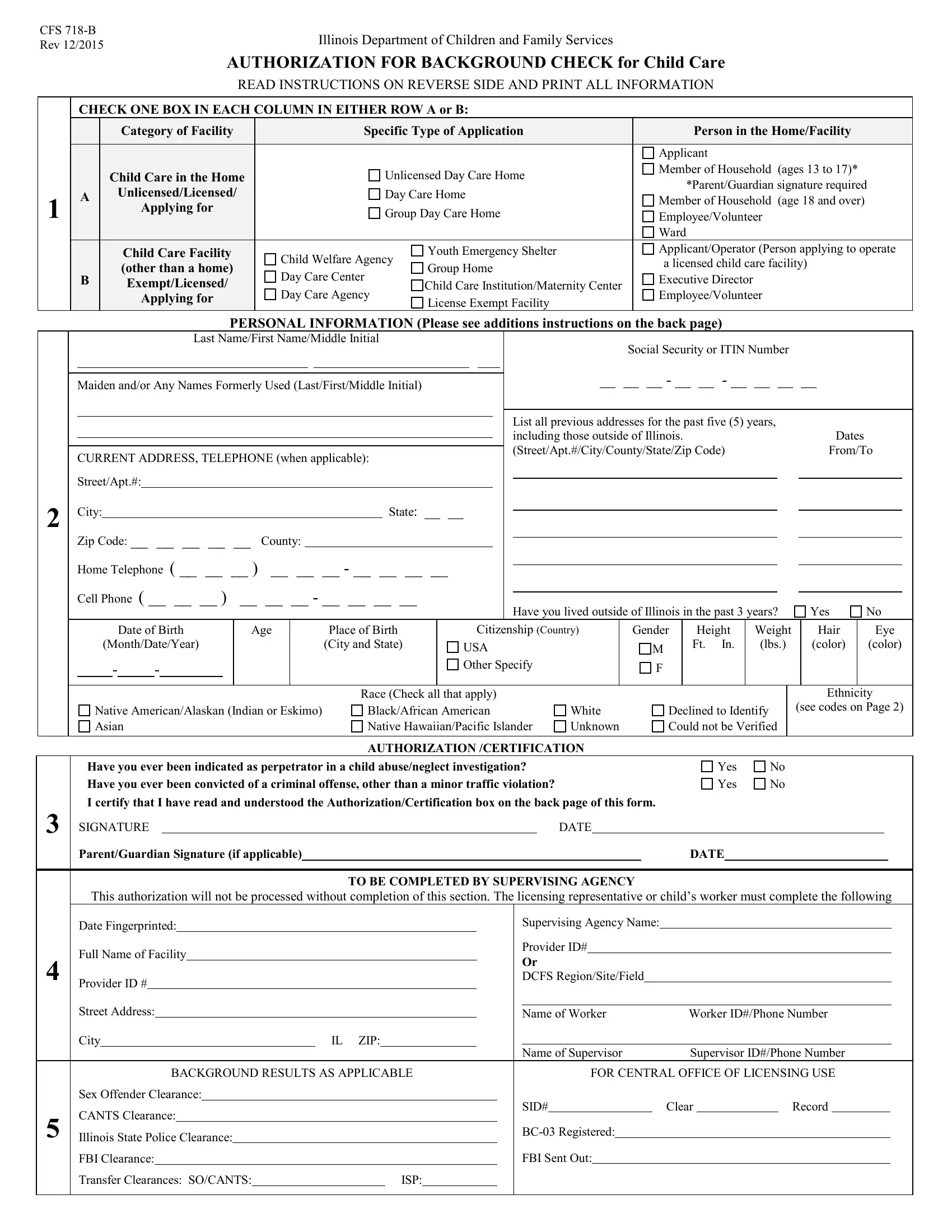
1. It is crucial to fill out the il background check form correctly, so be mindful when working with the areas including all these fields:
2. Once the last selection of blank fields is completed, go to enter the relevant details in these: Home Telephone, Cell Phone, Date of Birth, MonthDateYear, Age, Place of Birth City and State, Have you lived outside of Illinois, Yes, Citizenship Country, Gender, USA, Other Specify, Height Ft In, Weight lbs, and Hair.
You can certainly make an error while filling out the Home Telephone, consequently ensure that you go through it again before you send it in.
Step 3: Check that your information is accurate and then click "Done" to continue further. Go for a free trial plan with us and get direct access to il background check form - which you'll be able to then work with as you wish in your personal account. We don't share or sell the details you provide while completing forms at FormsPal.