
Any time you desire to fill out uscg dot form, you don't need to download any kind of programs - simply use our PDF editor. Our editor is continually developing to present the very best user experience possible, and that is because of our resolve for continuous improvement and listening closely to feedback from users. Here is what you would need to do to begin:
Step 1: Access the form inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: With this advanced PDF editing tool, you're able to accomplish more than simply fill in blank form fields. Express yourself and make your forms seem sublime with custom textual content added in, or optimize the file's original input to perfection - all that supported by the capability to insert your own images and sign it off.
Completing this form requires focus on details. Ensure that all necessary blanks are filled out correctly.
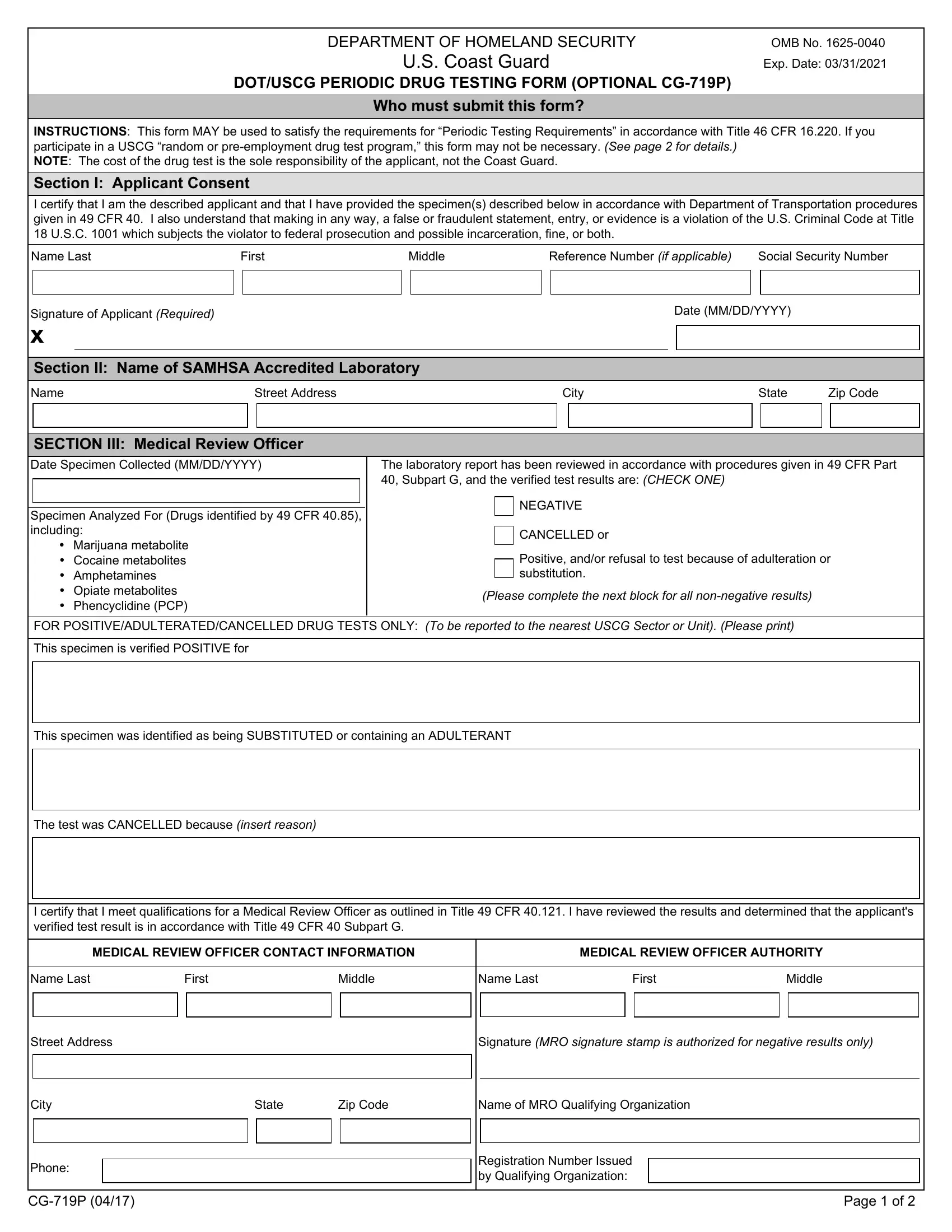
1. Begin filling out your uscg dot form with a number of major blank fields. Gather all of the information you need and make sure nothing is forgotten!
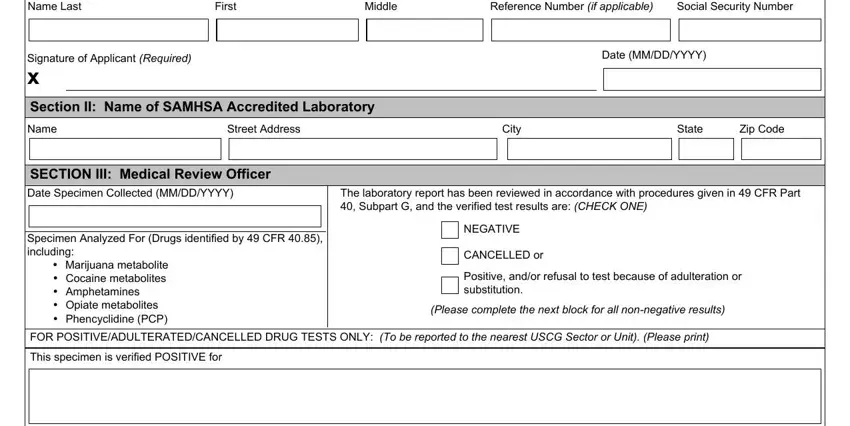
2. Soon after this part is done, proceed to type in the applicable details in all these - This specimen was identified as, The test was CANCELLED because, I certify that I meet, MEDICAL REVIEW OFFICER CONTACT, MEDICAL REVIEW OFFICER AUTHORITY, Name Last, First, Middle, Name Last, First, Middle, Street Address, Signature MRO signature stamp is, City, and Phone.
People generally make errors when filling in Signature MRO signature stamp is in this part. Ensure you read twice everything you type in right here.
Step 3: Prior to moving on, check that blanks were filled in the correct way. As soon as you are satisfied with it, click on “Done." Right after setting up a7-day free trial account at FormsPal, you'll be able to download uscg dot form or email it promptly. The PDF form will also be readily available through your personal account with your every single modification. FormsPal guarantees your information privacy with a secure system that in no way saves or distributes any type of personal information used in the form. Rest assured knowing your files are kept safe when you work with our services!