
Fill out the CG-719P drug testing form online using our free PDF editor. No software download is required. Follow these steps to complete your DOT/USCG Periodic Drug Testing Form accurately before submitting it to the USCG or your testing facility.
Step 1: Access the form inside our tool by pressing the "Get Form Button" at the top of this page.
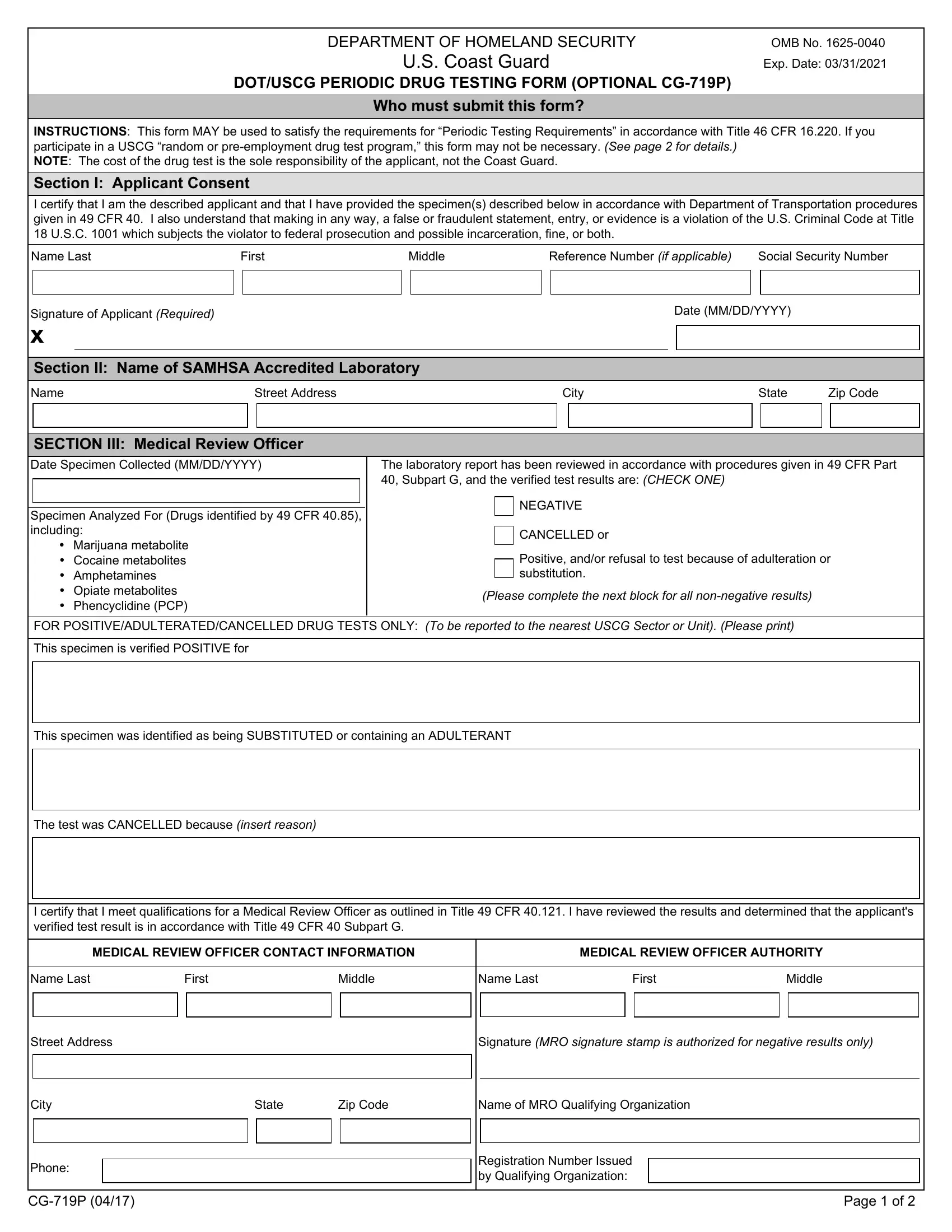
Step 2: Complete Section I with your personal details: full name, USCG credential number, date of birth, and the name of the SAMHSA-accredited laboratory conducting your test. Enter the specimen identification number provided at the collection site.
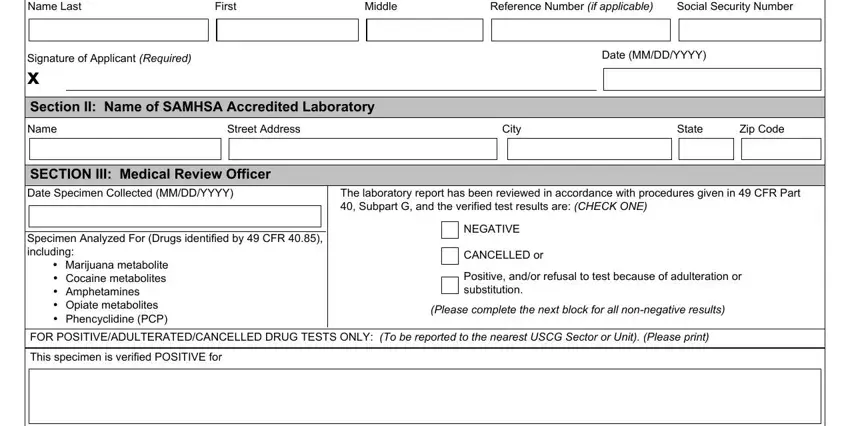
Step 3: Review Section II if applicable. This part is completed by the Medical Review Officer (MRO) after testing and must include the MRO name, contact details, authority information, and signature confirming the result meets DOT drug testing standards.
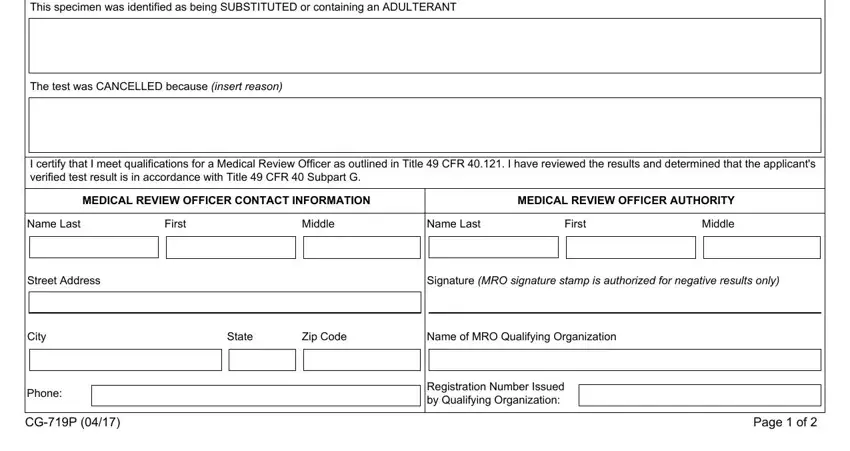
Step 4: Check every field carefully. Falsifying any information on this form, such as altering specimen IDs or MRO signatures, may result in federal prosecution.
Step 5: Click "Done" to save. You can then download a printable PDF, email it, or store it in your FormsPal account. Your data stays private and is never shared beyond your session.
Frequently Asked Questions About the CG-719P Form
What is the CG-719P form used for?
The CG-719P is the DOT/USCG Periodic Drug Testing Form. Mariners not covered by an employer-run random drug testing program use it to satisfy periodic testing requirements under 46 CFR 16.220 when renewing or applying for a Merchant Mariner Credential.
Who needs to submit the CG-719P?
Licensed officers, deck ratings, and STCW certificate holders who are not enrolled in a USCG-approved random testing program must complete the CG-719P. The applicant pays for testing and must use a SAMHSA-accredited laboratory.
What is the difference between CG-719P and CG-719B?
The CG-719B form is for initial MMC credential applications. The CG-719P is for periodic drug testing renewals where the mariner is not in a random testing program. The CG-719S form handles pre-employment and follow-up drug tests.
What laboratory must I use for the CG-719P drug test?
The test specimen must be analyzed by a SAMHSA-accredited laboratory. Provide the lab name and contact information in Section I of the form. A drug testing consent form may be required by the collection facility before testing begins.
Can I fill out the CG-719P online for free?
Yes. Use the PDF editor at the top of this page to complete all fields digitally and download a ready-to-submit copy at no cost. For related forms, explore the drug-free workplace certification and other compliance documents available on FormsPal.