Are you moving soon? If so, you'll need to fill out a Change of Address Form with the United States Postal Service. The form can be downloaded from the USPS website, or you can pick one up at your local post office. The process is fairly simple, but there are a few things you should know before completing the form. In this blog post, we'll walk you through the steps of filling out a Change of Address Form and provide some tips for making the move as smooth as possible. Let's get started!
| Question | Answer |
|---|---|
| Form Name | Change Of Address Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | humana com change of address, humana provider change of address form, humana provider address change, humana address change |
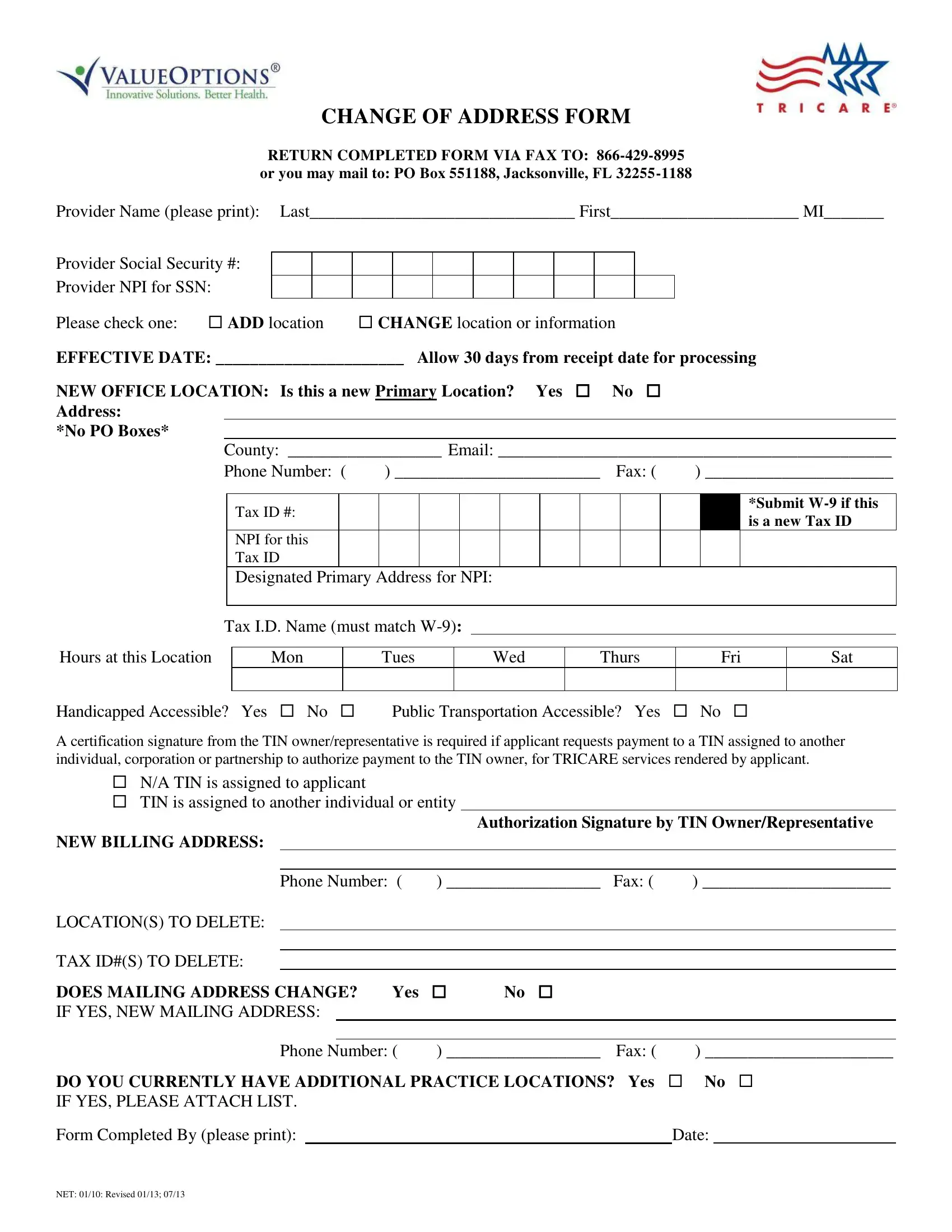
CHANGE OF ADDRESS FORM
RETURN COMPLETED FORM VIA FAX TO:
Provider Name (please print): Last_______________________________ First______________________ MI_______
Provider Social Security #:
Provider NPI for SSN:
Please check one: ADD location CHANGE location or information
EFFECTIVE DATE: ______________________ Allow 30 days from receipt date for processing
NEW OFFICE LOCATION: Is this a new Primary Location? Yes No Address:
*No PO Boxes*
County: __________________ Email: ______________________________________________
Phone Number: ( |
) ________________________ Fax: ( |
) ______________________ |
Tax ID #:
NPI for this Tax ID
*Submit
Designated Primary Address for NPI:
Tax I.D. Name (must match
Hours at this Location
Mon
Tues
Wed
Thurs
Fri
Sat
Handicapped Accessible? Yes No Public Transportation Accessible? Yes No
A certification signature from the TIN owner/representative is required if applicant requests payment to a TIN assigned to another individual, corporation or partnership to authorize payment to the TIN owner, for TRICARE services rendered by applicant.
N/A TIN is assigned to applicant
TIN is assigned to another individual or entity
Authorization Signature by TIN Owner/Representative
NEW BILLING ADDRESS:
|
Phone Number: ( |
) __________________ |
Fax: ( |
) ______________________ |
|||||
LOCATION(S) TO DELETE: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
TAX ID#(S) TO DELETE: |
|
|
|
|
|
|
|
||
DOES MAILING ADDRESS CHANGE? Yes |
|
No |
|
|
|
|
|||
IF YES, NEW MAILING ADDRESS: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Phone Number: ( |
) __________________ |
Fax: ( |
) ______________________ |
|||||
DO YOU CURRENTLY HAVE ADDITIONAL PRACTICE LOCATIONS? Yes |
No |
||||||||
IF YES, PLEASE ATTACH LIST. |
|
|
|
|
|
|
|||
Form Completed By (please print): |
|
|
|
|
|
Date: |
|
||
NET: 01/10: Revised 01/13; 07/13