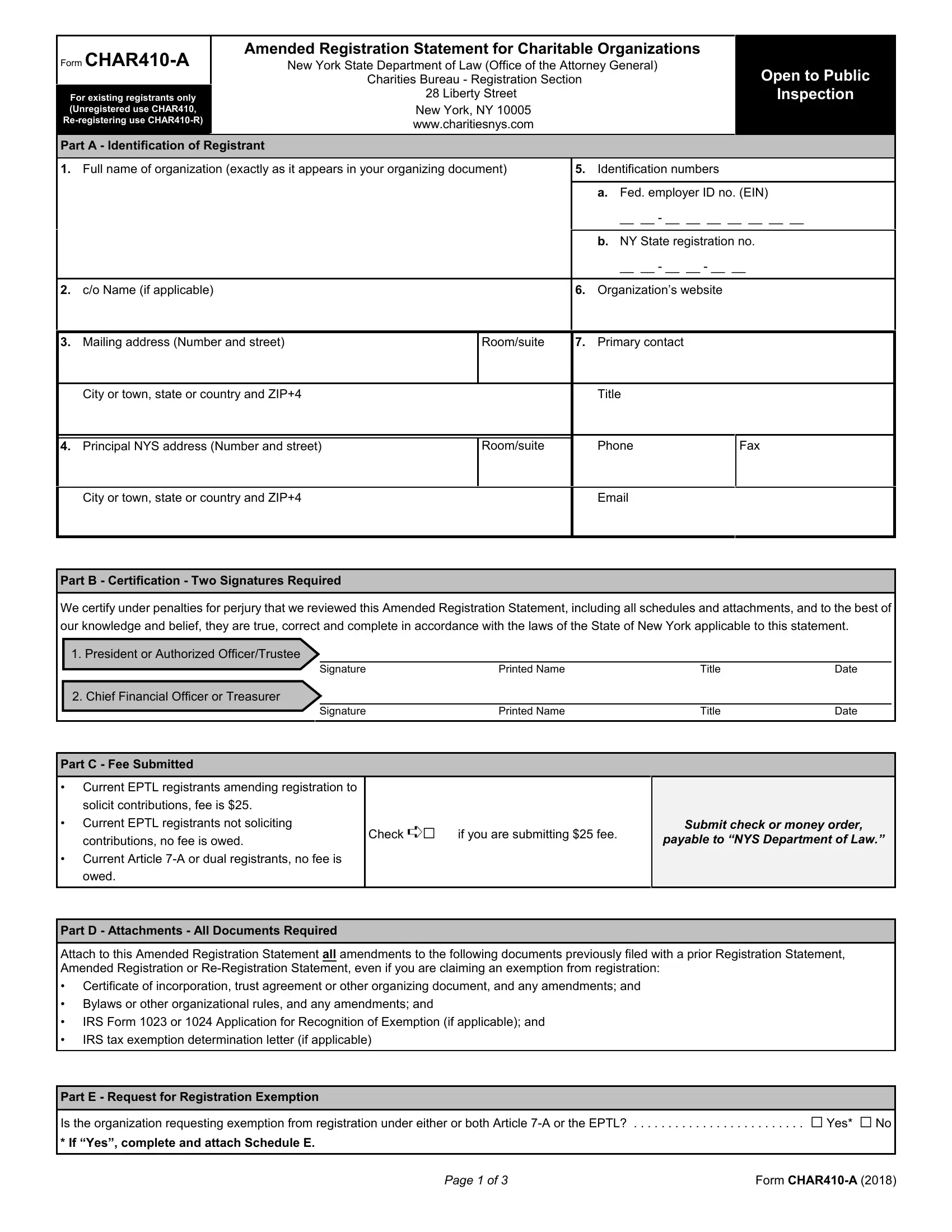
The CHAR410-A is the Amended Registration Statement for Charitable Organizations in New York State. It is filed with the New York State Department of Law's Charities Bureau. Existing registrants use this 3-page form to report changes to their registration information after the initial filing.
The CHAR410-A updates a charitable organization's existing registration with the Charities Bureau. It applies only to organizations already registered through the standard CHAR410 form. The form covers changes to the organization's legal identity, activities, and key personnel.
All statements on the CHAR410-A are certified under penalties of perjury. Senior officials must sign the certification section before submission.
Any registered charitable organization in New York State must file CHAR410-A to report changes. Common situations that require an amendment include:
Organizations that have not yet registered with the Bureau must file the initial CHAR410 form instead. The CHAR410-A is only for those with an existing registration number.
The form requires disclosure in three main areas. First, identification details such as the organization name, address, and EIN. Second, organizational activities including any revision to the charitable purpose or programs offered. Third, key personnel changes covering new or departing officers, directors, or trustees.
The form also includes a section for changes related to solicitation activities. Organizations that recently began or stopped soliciting donations in New York must check the applicable boxes and provide details.
To fill out the CHAR410-A, follow these steps:
Use FormsPal's free PDF editor to complete all fields before printing. The editor works in your browser without any software downloads.
The filing fee depends on the organization's registration status and its current solicitation activities. Fees are set by the Charities Bureau and may change from year to year. Organizations claiming an exemption from registration fees must submit a written exemption request along with the completed form.
Always check the current Charities Bureau fee schedule before submitting to make sure you include the correct amount. An incorrect fee can delay processing of your amendment.
Most amendments require supporting documentation. Common attachments include updated articles of incorporation, board resolutions that approved the change, and amended bylaws. The CHAR410-A instructions specify which attachments apply to each category of amendment.
Gather all required documents before filling out the form. Missing attachments are the most common reason for processing delays. Review the instructions for each amendment type you are checking on the form.
What is the difference between CHAR410 and CHAR410-A?
Form CHAR410 is the initial registration form for new charitable organizations in New York. The CHAR410-A is used only by organizations that are already registered and need to report changes to their existing registration details.
How long does the Charities Bureau take to process CHAR410-A?
Processing times vary. Most amendments are reviewed within 30 to 60 days of receipt. Contact the Charities Bureau directly to check the status of a specific filing.
What happens if I miss the deadline to file an amendment?
Failing to report a change on time can result in late fees or penalties from the Charities Bureau. File the CHAR410-A as soon as a reportable change occurs in your organization.
What other forms may I need with CHAR410-A?
If your organization is due for annual renewal, you may also need the CHAR410-R renewal registration form. Organizations tracking financial details for their Charities Bureau filings can use the charitable worksheet to organize their information.
| Question | Answer |
|---|---|
| Form Name | Char410 A Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | char410a, char 410 2018 pdf, char 410 a, f organization registration |