
You are able to complete subject chrc form instantly with our PDFinity® online PDF tool. We are aimed at making sure you have the ideal experience with our editor by continuously releasing new functions and improvements. With all of these updates, working with our editor becomes easier than ever! To start your journey, take these simple steps:
Step 1: Open the PDF form in our editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: This editor provides the ability to work with your PDF form in a variety of ways. Transform it by adding customized text, correct what's originally in the document, and include a signature - all doable in no time!
This PDF form requires particular info to be filled out, thus you should definitely take your time to enter what is expected:
1. It's very important to complete the subject chrc form correctly, so be mindful when filling out the segments that contain these blank fields:
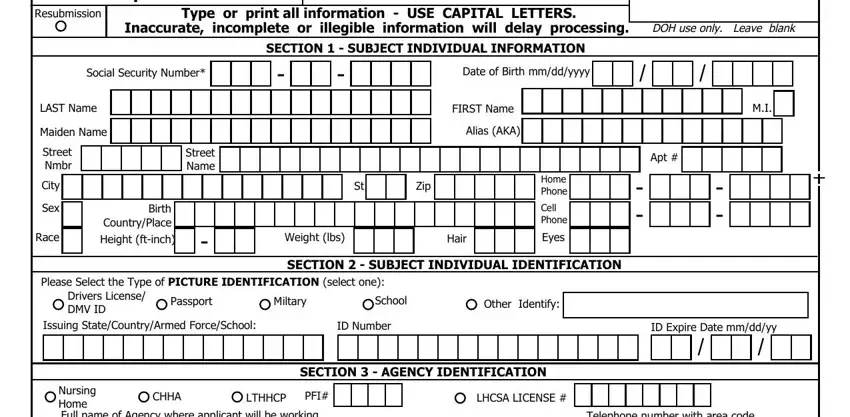
2. Soon after finishing the last part, go on to the next part and enter the necessary details in these fields - Nursing Home Full name of Agency, Authorized Person LAST Name, Agencys Street Nmbr, City, Authorized Partys email, Street Name, FIRST Name, Telephone number with area code, State, Zip, The subject individual whose, Signature of Agency Authorized, Date, SECTION FINGERPRINTING, and Fingerprint Method.
Regarding Nursing Home Full name of Agency and FIRST Name, make certain you take a second look here. Those two are thought to be the most significant fields in this file.
Step 3: Before submitting the document, make sure that all form fields have been filled out right. When you determine that it is fine, click “Done." Right after setting up afree trial account here, you will be able to download subject chrc form or email it at once. The PDF will also be at your disposal through your personal account page with all your adjustments. Here at FormsPal.com, we strive to make certain that all your details are stored private.