Completing the Cigna provider appeal form is straightforward with our online editor. Follow these steps:
Step 1: Click the orange "Get Form Now" button to open the form editor.
Step 2: On the editing page, you can add or update information, highlight text, insert checks or signatures, and remove fields as needed.
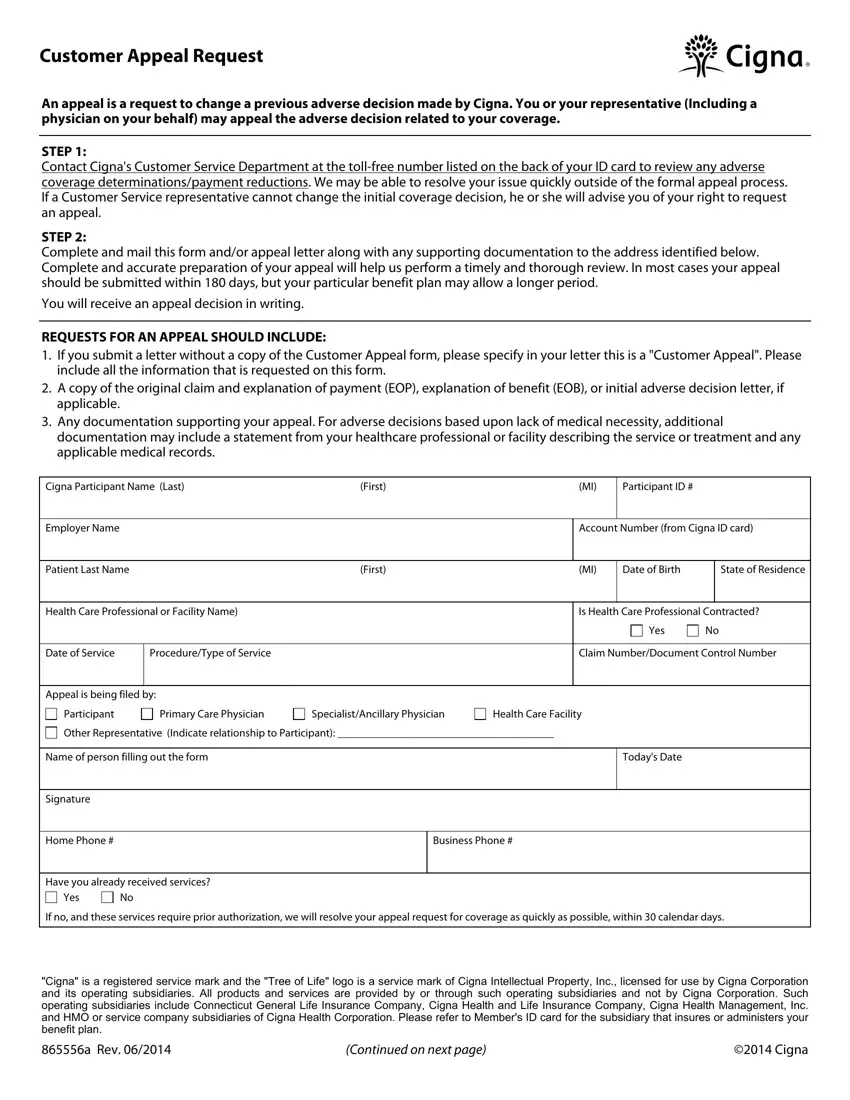
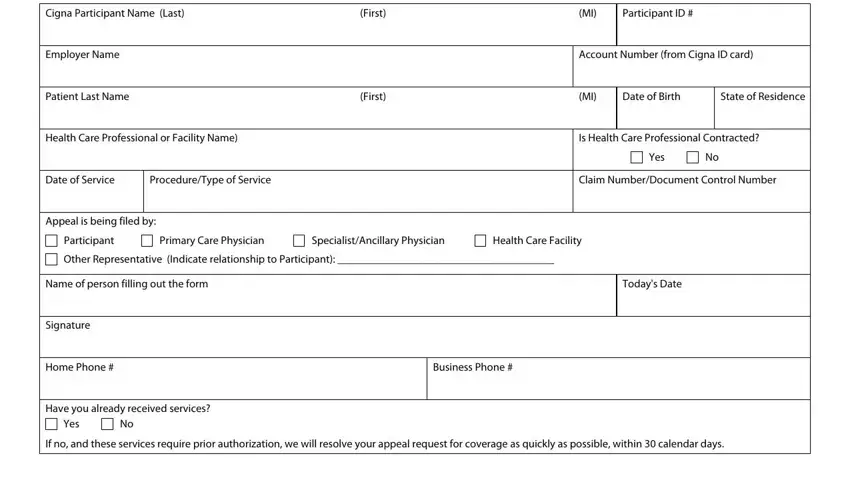
The following sections appear in the PDF document you will be completing.
Enter the required information in the appeal type area. Select the appropriate reason: Request for in-network coverage, Coverage Exclusion or Limitation, Maximum Reimbursable Amount, Inpatient Facility Denial Level of Care, Mutually Exclusive or Incidental, Additional reimbursement, Experimental or Investigational, Medical Necessity, Timely Claim Filing without proof, Benefits reduced due to repricing, or the reason you believe the adverse decision was incorrect.
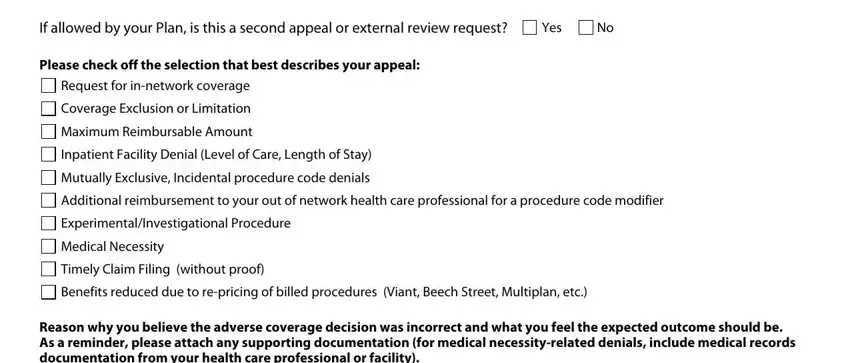
In the section for Reason why you believe the adverse decision is incorrect and Additional Comments, provide a detailed explanation supported by medical or policy evidence.
The signature section requires both parties to acknowledge the rights and obligations involved in the appeal.

Step 3: Click "Done" to finalize the form. Save it to your device or send it directly by email.
Step 4: Create duplicates of your completed form for your records. Your personal information is never shared or tracked.
What to Include in Your Appeal
A thorough submission improves your chances of a favorable decision. Gather these items before submitting your appeal:
- The original denial letter or Explanation of Benefits (EOB)
- Your member ID, provider name, and date of service
- Medical records, lab results, or physician notes supporting medical necessity
- A Letter of Medical Necessity from your treating provider, if applicable
- Prior authorization documentation, if one was requested
- Proof of payment for reimbursement disputes
Common Reasons to File an Insurance Appeal
Cigna members appeal decisions for a variety of reasons. The most frequent include:
- Medical necessity denial - a treatment or service was deemed not medically necessary
- Out-of-network charge disputes - in-network providers were unavailable in your area
- Coverage exclusion challenges - a service was denied under a plan exclusion
- Timely filing denials - a claim was submitted outside the standard window
- Experimental treatment decisions - a treatment was classified as investigational
- Repricing disputes - reimbursement was reduced below the expected contracted rate
Tips for a Stronger Appeal
Increase your chance of approval with these steps:
- Submit within 180 days of the denial to meet the filing deadline
- Reference the exact policy language or benefit provision you are disputing
- Request expedited review for urgent or life-threatening medical situations
- Ask your physician to write a supporting letter directly addressed to Cigna
- Keep a complete copy of your appeal packet and all attached documents
- If the internal appeal is denied, you may request an independent external review
Frequently Asked Questions
How long do I have to file a Cigna appeal?
You must file within 180 days of receiving the adverse benefit decision. Some plans allow a longer window - review your benefit plan documents for the exact deadline.
Can someone else file the appeal on my behalf?
Yes. A physician, provider, or authorized representative may file on your behalf. Include a signed authorization form with your submission.
How long does Cigna take to decide an appeal?
Standard appeals are typically decided within 30 days for pre-service claims and 60 days for post-service claims. Expedited appeals for urgent care are decided within 72 hours.
What if my appeal is denied?
You may request an external independent review by a reviewer not affiliated with Cigna. This right is protected under federal and state law for most group health plans.
Related Insurance Appeal Forms
Looking for other appeal and insurance claim forms? Browse these related resources:
