We were creating this PDF editor having the idea of making it as effortless make use of as possible. That's the reason the entire process of filling in the cigna botox prior auth form will likely to be smooth use all of these steps:
Step 1: To begin, hit the orange button "Get Form Now".
Step 2: Now you are allowed to manage cigna botox prior auth form. You have a wide range of options with our multifunctional toolbar - you can include, eliminate, or alter the information, highlight the particular sections, as well as conduct many other commands.
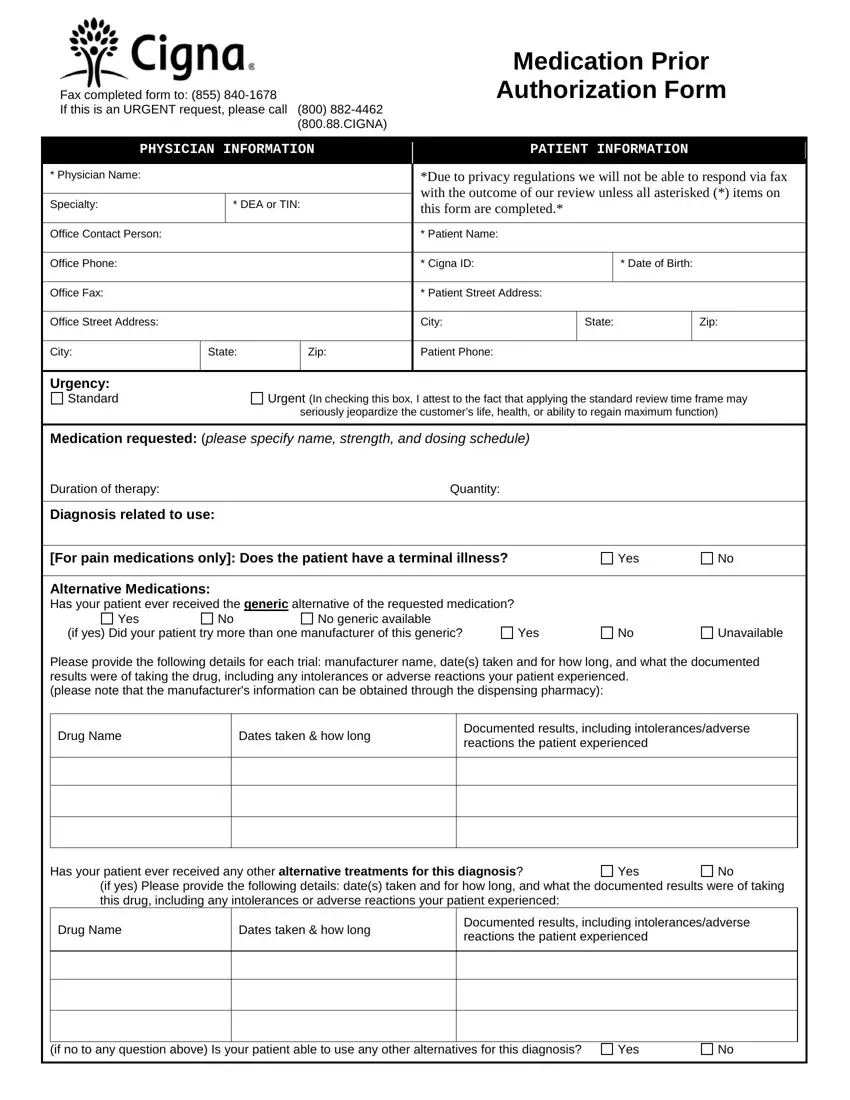
Provide the required content in every single part to complete the PDF cigna botox prior auth form
Within the box Alternative Medications Has your, Yes, No generic available, if yes Did your patient try more, Yes, Unavailable, Please provide the following, Drug Name, Dates taken how long, Documented results including, Has your patient ever received any, Yes, if yes Please provide the, Drug Name, and Dates taken how long type in the data the application requests you to do.
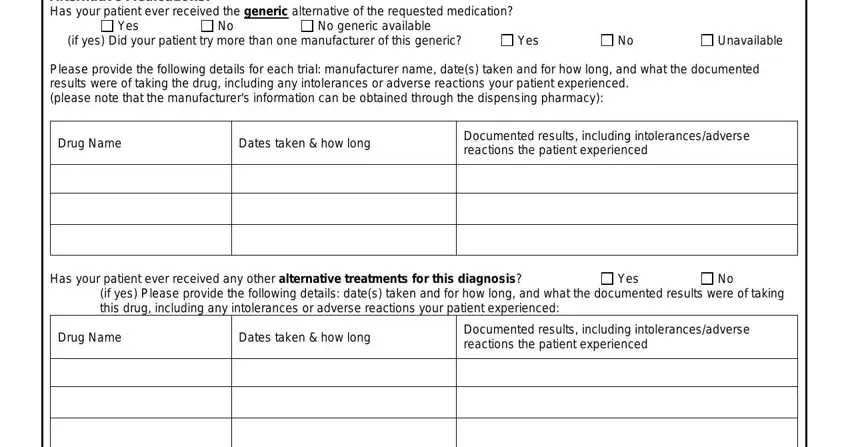
The application will require for further details in order to easily fill in the section if no to any question above Is, and Yes.

Identify the rights and responsibilities of the parties within the space Save Time Submit Online at, Our standard response time for, and Cigna is a registered service mark.
Step 3: Select the Done button to be sure that your completed form is available to be transferred to each gadget you decide on or sent to an email you indicate.
Step 4: Create at least several copies of your document to keep away from any possible future challenges.
