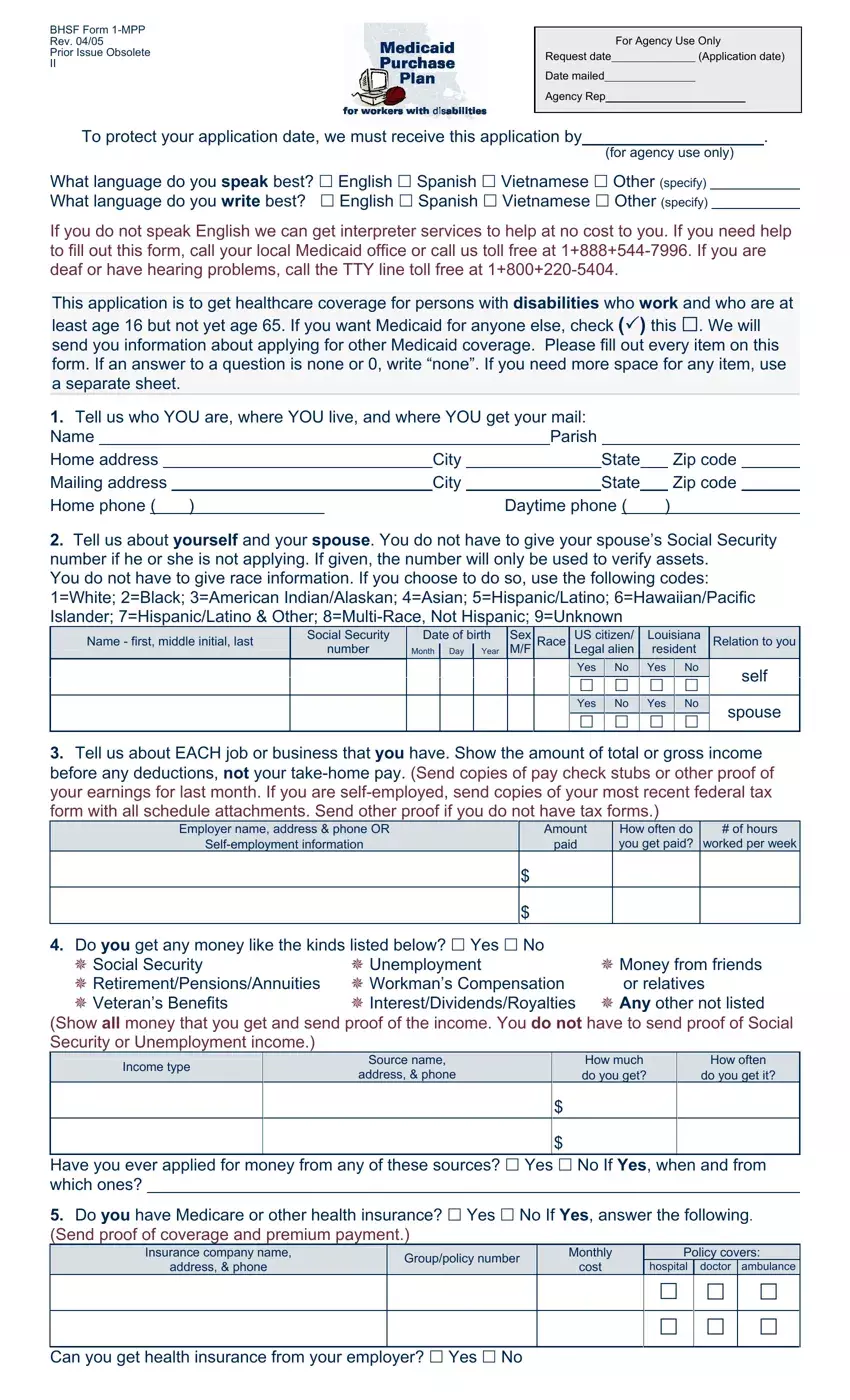
Before you begin, gather everything you will need to complete the application. You should have your Social Security card, proof of income, health insurance information, a list of your financial assets, and contact details for your healthcare providers. Having these items ready before you start will help you avoid stopping partway through.
Step 1: Click the orange "Get Form Now" button at the top of this page. This opens the application in our free online PDF editor.
Step 2: Review the toolbar at the top of the editing screen. You can use these tools to type in the form fields, check boxes, add dates, and apply a digital signature.
Start by filling in the personal information section. This is the first part of the form and asks for your basic details.
In the first section, complete each of these fields:
- Your full name (first name, middle initial, last name)
- Your daytime phone number
- Your Social Security number
- Your date of birth (month, day, year)
- Sex (male or female)
- Race and ethnicity
- Citizenship or immigration status (US citizen or legal alien)
- State residency confirmation
- Your relationship to the primary applicant, if you are filling this out on behalf of someone else
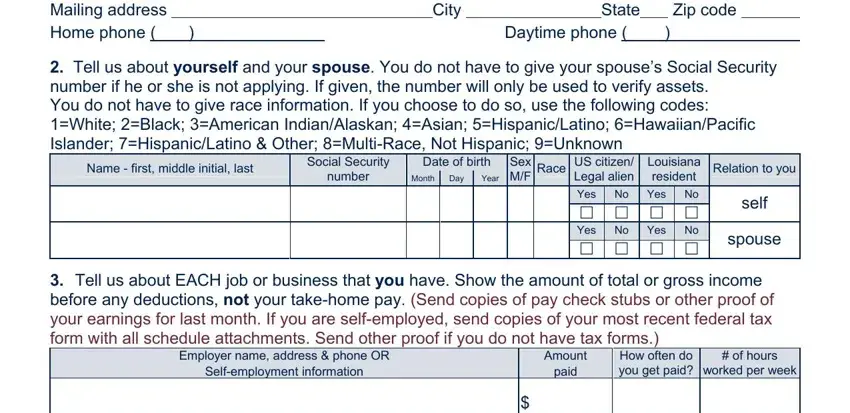
Next, move to the income and financial resources section. You must report all sources of money you receive. Be accurate and complete. Incomplete income information is one of the most common reasons applications are delayed or denied.
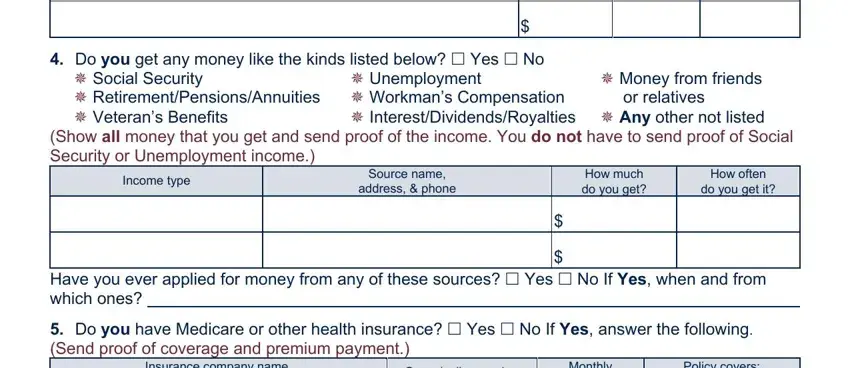
Complete each of the following income fields:
- Interest, dividends, or royalties received
- Money from friends or relatives
- Unemployment benefits, if applicable
- Income type and source name, address, and phone
- How much you receive and how often
- Whether you have applied for other financial assistance before
- Medicare or other health insurance coverage details
In the health insurance section, list all current policies. Include both private insurance and any employer-sponsored coverage. For each policy, enter:
- Insurance company name and mailing address
- Group number and policy number
- Monthly premium cost
- What the policy covers (hospital, doctor visits, ambulance, other)
- Whether you can get health insurance through your employer

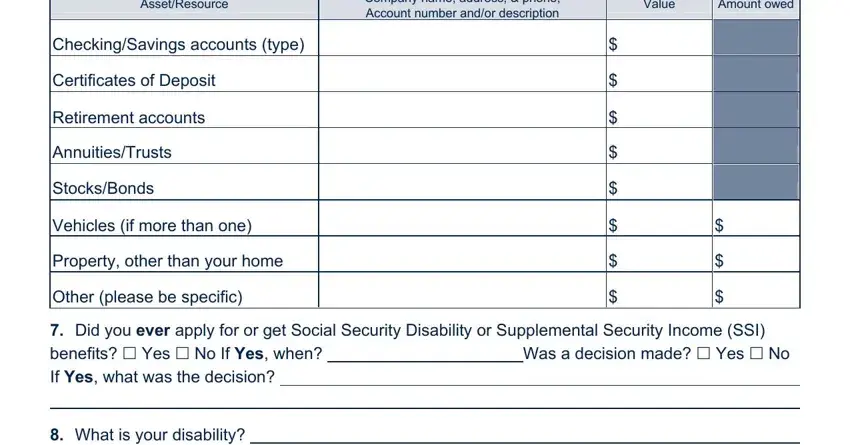
Next, complete the assets and resources section. You must list all financial assets, including those held jointly with another person. Include all of the following:
- Company names and contact information for each institution
- The current value and any amount still owed on each asset
- Checking and savings accounts
- Certificates of deposit
- Retirement accounts (401k, IRA, or pension funds)
- Annuities and trusts
- Stocks and bonds
- Vehicles if you own more than one
- Property other than your primary home
- Any other significant assets or resources
- A description of your disability
Step 3: Once all sections are complete, click the Done button. You can then export the finished document to your computer or send it to an email address of your choice.
Step 4: Print and sign the completed form. Make at least two copies before submitting. Keep one copy for your personal records. Submit the signed original to your local AHCCCS office or Care 1st Arizona plan office.
Frequently Asked Questions
Do I need to submit supporting documents with the form?
Yes. You should attach proof of identity, proof of income, and documentation of your health insurance status. AHCCCS may request additional records during the review process.
How do I know if my application was received?
AHCCCS will mail you a confirmation notice after receiving your application. If you do not receive a confirmation within 10 business days of submitting, contact your local AHCCCS office to follow up.
What happens after my application is approved?
If approved, you will be enrolled in a Medicaid managed care plan. In Arizona, this may be Care 1st Arizona or another AHCCCS plan available in your area. You will receive a member ID card and information about how to access your new coverage.
Can I appeal if my application is denied?
Yes. You have the right to appeal a denial. The denial notice will explain the reason and include instructions on how to file an appeal. You must submit the appeal within the deadline stated in the notice.
