This PDF editor allows you to complete the Cigna Prior Authorization Form directly in your browser. The steps below walk through each section so the form is filled out accurately and completely.
Step 1: Open the form
Click the orange "Get Form Now" button at the top of this page. The PDF editor launches without any download or installation required.
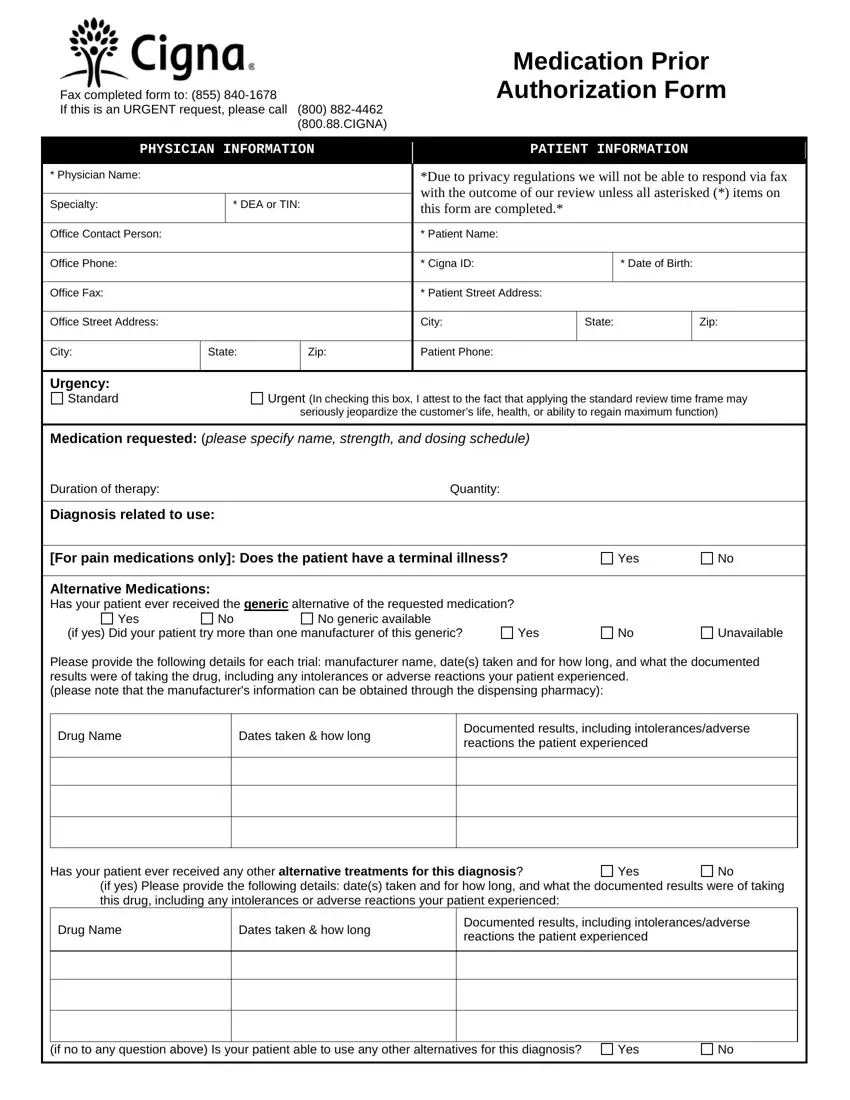
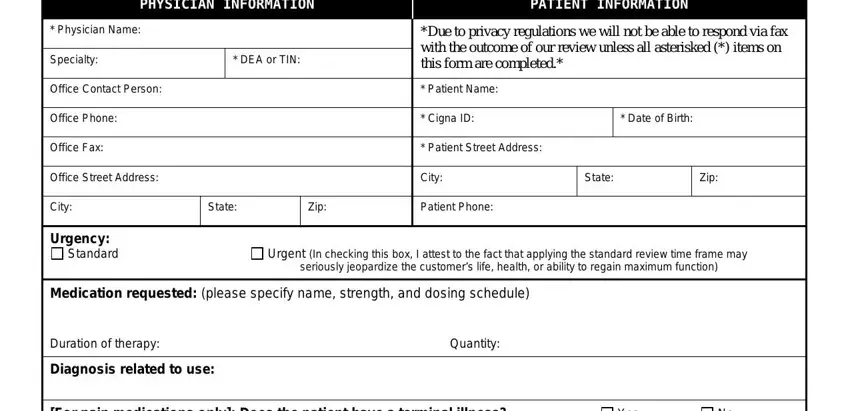
Step 2: Enter prescriber and patient information
Provide the prescribing physician's name, NPI number, fax number, and office phone number. Then enter the patient's full name, Cigna member ID, date of birth, and the relevant ICD-10 diagnosis code. Complete and accurate information in this section prevents processing delays.
Step 3: Document the requested medication or treatment
Specify the drug name, dosage, strength, and quantity requested. For specialty medications such as Botox injections, include the medical indication and any supporting clinical notes describing the patient's condition.
Step 4: Complete the alternative medications section
List any prior medications or generic alternatives the patient has already tried. For each, include the drug name, dates of use, and the clinical outcome or reason for discontinuation. Cigna uses this information when reviewing the authorization request.
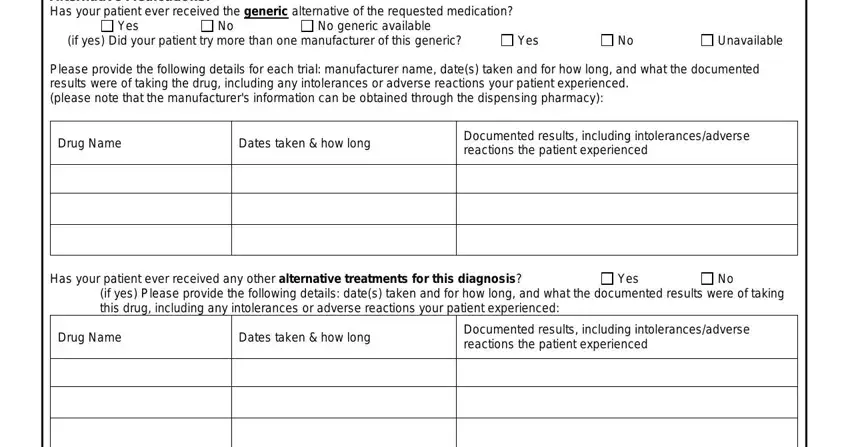
In the section asking whether any question above applies, mark Yes or No and complete the follow-up fields as required.

Step 5: Select the review type
Check the appropriate box for standard or urgent review. Urgent review applies when delaying treatment could seriously harm the patient. Standard prescription drug coverage requests are processed within five business days. Submit the completed form by fax to the number shown on the form, or use CoverMyMeds or SureScripts for electronic submission.
Step 6: Save and distribute the completed form
Click the Done button when all sections are filled in. Download the finished form or send it directly to an email address. Keep a copy for the patient's medical record and the prescribing physician's files.
Looking for other prior authorization forms? See the Cigna Appeal Form for denied requests, the Aetna Pharmacy Prior Authorization Form, or the Antipsychotic Prior Authorization Form.
