


When you want to fill out nys 55b c application, you don't have to install any kind of software - simply try our online tool. The editor is constantly improved by our staff, receiving awesome features and turning out to be greater. To get the process started, consider these easy steps:
Step 1: Open the PDF file inside our tool by clicking on the "Get Form Button" in the top section of this webpage.
Step 2: When you launch the editor, you will see the form ready to be completed. In addition to filling in various fields, you could also perform some other things with the PDF, particularly writing any text, editing the initial textual content, inserting graphics, placing your signature to the document, and a lot more.
For you to finalize this PDF form, make certain you type in the necessary information in every blank:
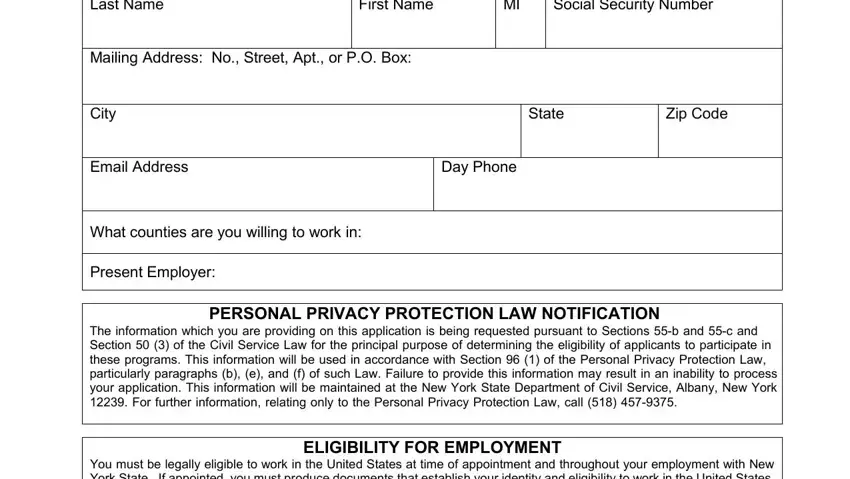
1. Complete your nys 55b c application with a group of major blank fields. Consider all of the information you need and make sure absolutely nothing is forgotten!
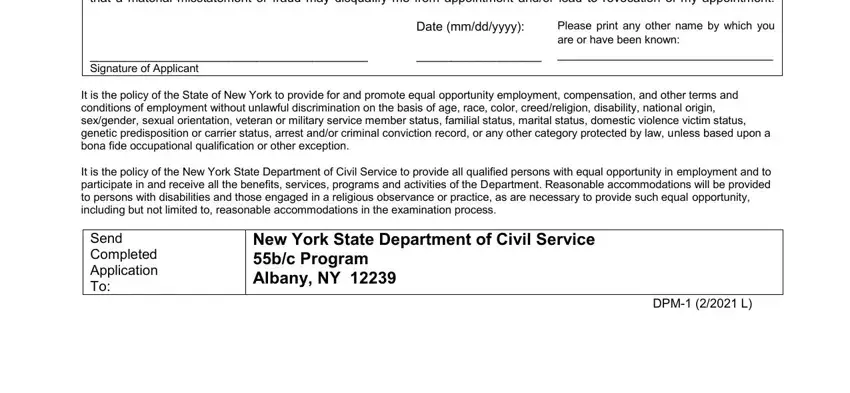
2. After finishing the previous step, head on to the subsequent stage and enter all required details in these blanks - I affirm under penalties of, Signature of Applicant, Date mmddyyyy, Please print any other name by, It is the policy of the State of, It is the policy of the New York, Send Completed Application To, New York State Department of Civil, and DPM L.
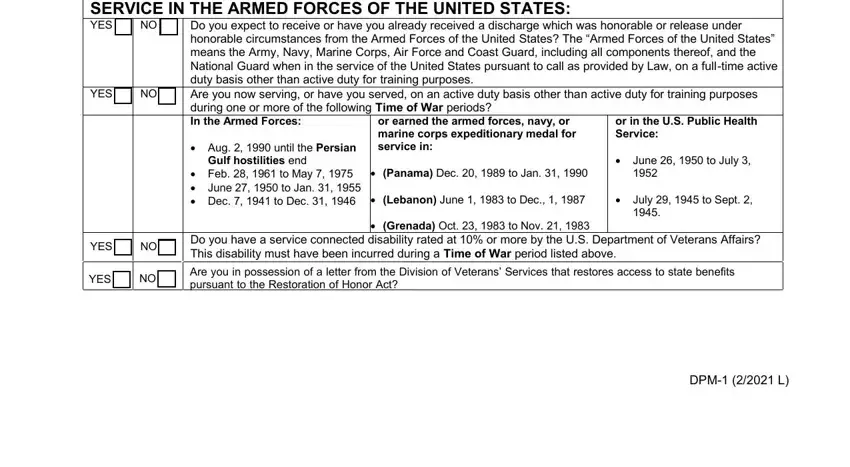
3. In this specific stage, examine SERVICE IN THE ARMED FORCES OF THE, Do you expect to receive or have, YES, Aug until the Persian, Gulf hostilities end, Feb to May June to Jan, or earned the armed forces navy or, or in the US Public Health Service, Panama Dec to Jan, Lebanon June to Dec, Grenada Oct to Nov, June to July, July to Sept, YES, and YES. Each one of these must be filled in with highest focus on detail.
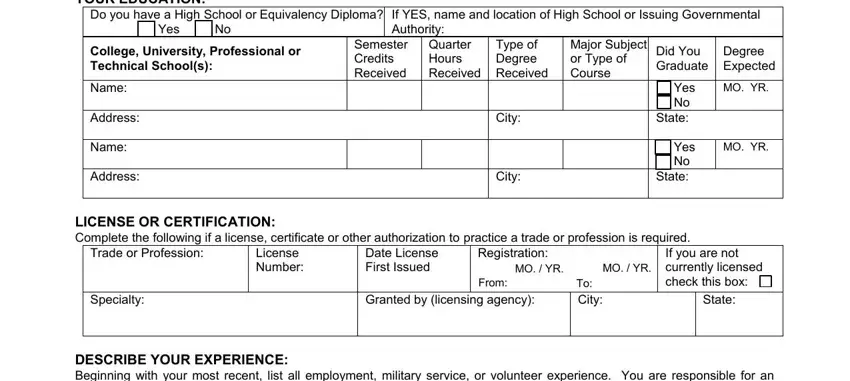
4. The subsequent part will require your attention in the subsequent areas: YOUR EDUCATION, Do you have a High School or, Yes, If YES name and location of High, College University Professional or, Semester Credits Received, Quarter Hours Received, Type of Degree Received, Major Subject or Type of Course, Did You Graduate, Degree Expected, Name, Address, Name, and Address. Remember to give all of the requested details to move further.
5. Because you approach the conclusion of the form, there are several more requirements that need to be fulfilled. Particularly, LENGTH OF EMPLOYMENT, MO YR, MO YR, From, FIRM NAME ADDRESS CITY AND STATE, DUTIES, TYPE OF BUSINESS, YOUR EXACT TITLE, NAME OF YOUR SUPERVISOR, SUPERVISORS TITLE, No of hours worked per week, LENGTH OF EMPLOYMENT, MO YR, MO YR, and From must all be done.
Always be really attentive while filling in DUTIES and MO YR, since this is the section in which many people make some mistakes.
Step 3: Confirm that the information is correct and click on "Done" to progress further. Get the nys 55b c application after you join for a 7-day free trial. Immediately view the form in your FormsPal cabinet, with any edits and changes conveniently synced! Here at FormsPal.com, we strive to make sure that your details are maintained private.