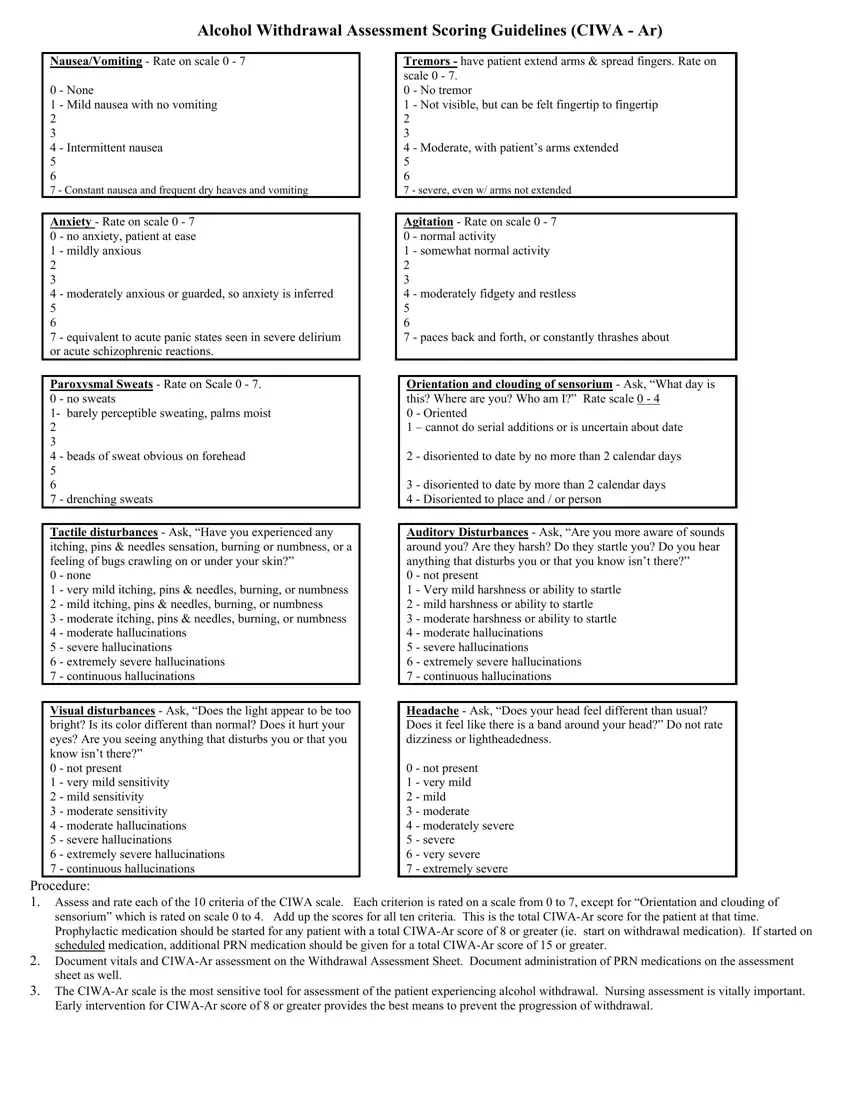
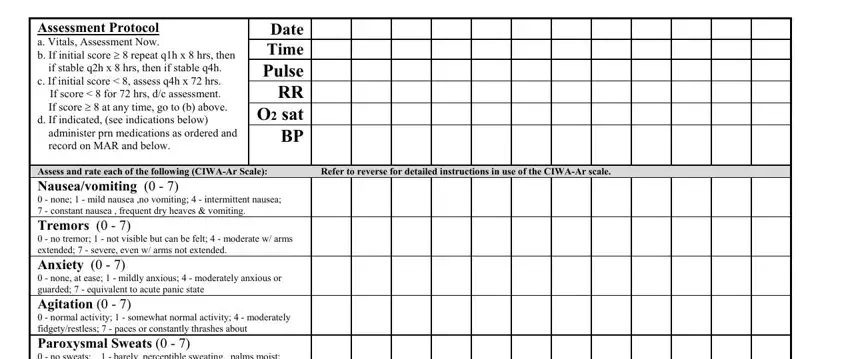
Nausea/Vomiting - Rate on scale 0 - 7
0 - None
1 - Mild nausea with no vomiting
2
3
4 - Intermittent nausea
5
6
7 - Constant nausea and frequent dry heaves and vomiting
Anxiety - Rate on scale 0 - 7
0 - no anxiety, patient at ease
1 - mildly anxious
2
3
4 - moderately anxious or guarded, so anxiety is inferred 5 6
7 - equivalent to acute panic states seen in severe delirium or acute schizophrenic reactions.
Paroxysmal Sweats - Rate on Scale 0 - 7.
0 - no sweats
1- barely perceptible sweating, palms moist
2
3
4 - beads of sweat obvious on forehead
5
6
7 - drenching sweats
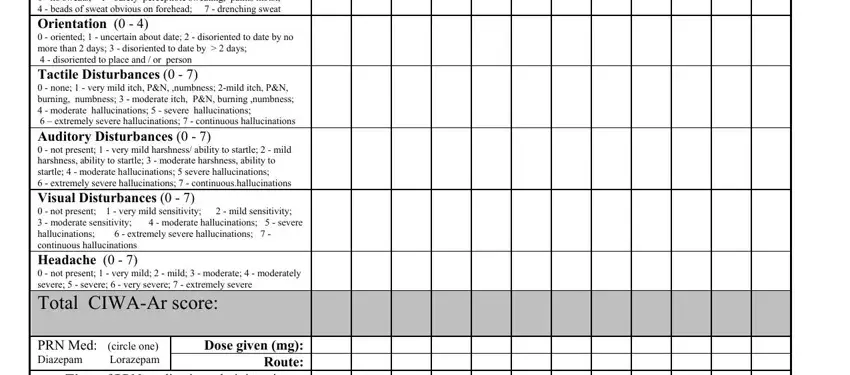
Tactile disturbances - Ask, “Have you experienced any itching, pins & needles sensation, burning or numbness, or a feeling of bugs crawling on or under your skin?”
0 - none
1 - very mild itching, pins & needles, burning, or numbness 2 - mild itching, pins & needles, burning, or numbness
3 - moderate itching, pins & needles, burning, or numbness 4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Visual disturbances - Ask, “Does the light appear to be too bright? Is its color different than normal? Does it hurt your eyes? Are you seeing anything that disturbs you or that you know isn’t there?”
0 - not present
1 - very mild sensitivity
2 - mild sensitivity
3 - moderate sensitivity
4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Tremors - have patient extend arms & spread fingers. Rate on scale 0 - 7.
0 - No tremor
1 - Not visible, but can be felt fingertip to fingertip 2 3
4 - Moderate, with patient’s arms extended
5
6
7 - severe, even w/ arms not extended
Agitation - Rate on scale 0 - 7 0 - normal activity
1 - somewhat normal activity
2
3
4 - moderately fidgety and restless
5
6
7 - paces back and forth, or constantly thrashes about
Orientation and clouding of sensorium - Ask, “What day is this? Where are you? Who am I?” Rate scale 0 - 4
0 - Oriented
1 – cannot do serial additions or is uncertain about date
2 - disoriented to date by no more than 2 calendar days
3 - disoriented to date by more than 2 calendar days 4 - Disoriented to place and / or person
Auditory Disturbances - Ask, “Are you more aware of sounds around you? Are they harsh? Do they startle you? Do you hear anything that disturbs you or that you know isn’t there?”
0 - not present
1 - Very mild harshness or ability to startle
2 - mild harshness or ability to startle
3 - moderate harshness or ability to startle
4 - moderate hallucinations
5 - severe hallucinations
6 - extremely severe hallucinations
7 - continuous hallucinations
Headache - Ask, “Does your head feel different than usual? Does it feel like there is a band around your head?” Do not rate dizziness or lightheadedness.
0 - not present
1 - very mild
2 - mild
3 - moderate
4 - moderately severe
5 - severe
6 - very severe
7 - extremely severe