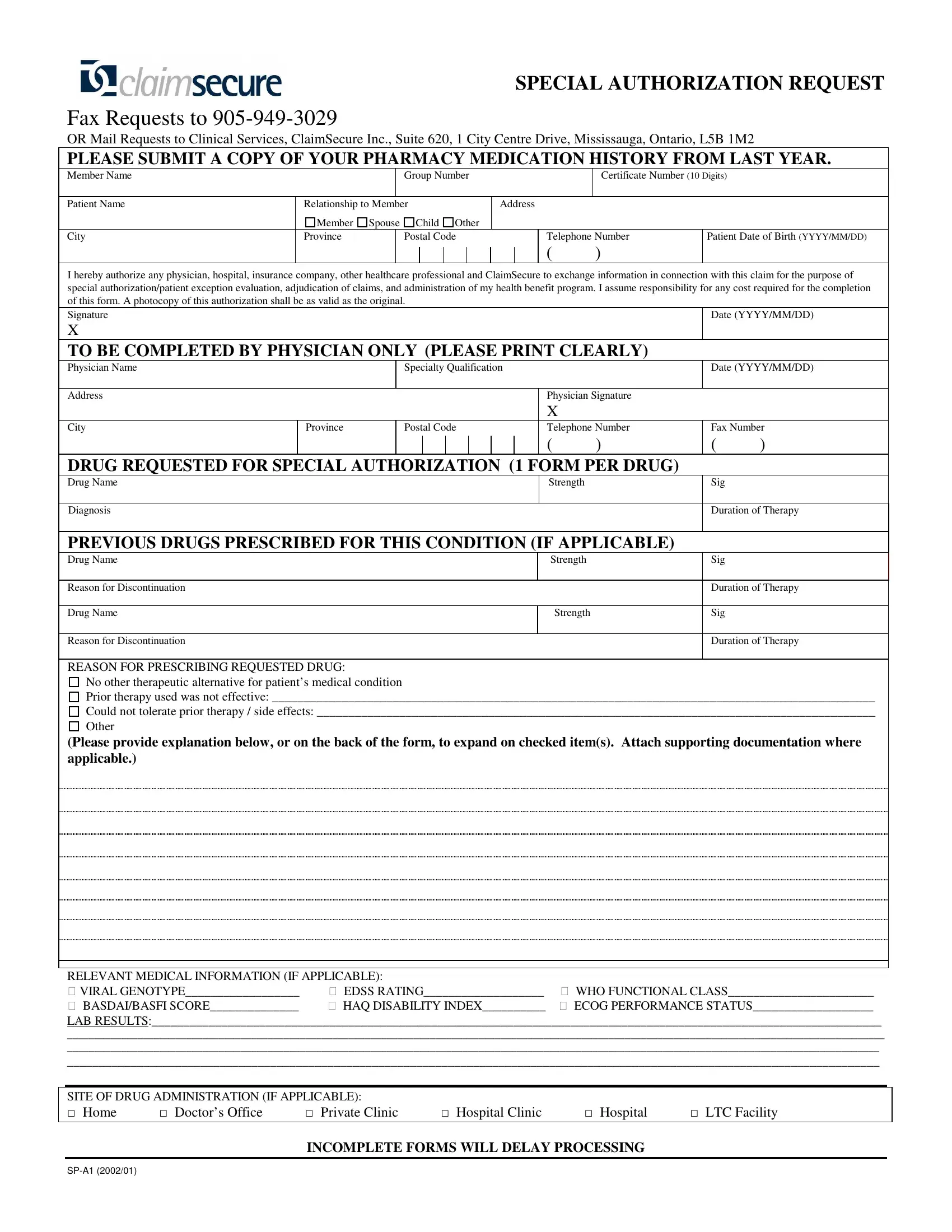
The ClaimSecure Sp A1 form serves a critical function in the healthcare management sphere, primarily designed to facilitate the process of obtaining special authorization for medication under a patient's health benefit program. This comprehensive document requires detailed input from both the patient and the prescribing physician, including patient personal information, medication history, and a specific drug request for special authorization. What sets this form apart is its meticulous approach to ensuring that all parties--from patients and doctors to pharmacies and ClaimSecure itself--can efficiently exchange necessary information for the evaluation and adjudication of claims. It puts a robust emphasis on the justification for the requested medication, whether due to the ineffectiveness of previous treatments, intolerance to other drugs, or the absence of alternative therapeutic options. By mandating a detailed pharmacy medication history and a thorough explanation for the drug request, the form aims to streamline the approval process, reducing delays and improving the accuracy of decisions made regarding patient care. Additionally, the form addresses the logistics of drug administration, allowing for a clear communication channel between healthcare providers and insurance professionals, which in turn, assures that patients receive the most appropriate and effective treatments without unnecessary hurdles.
| Question | Answer |
|---|---|
| Form Name | Claimsecure Form Sp A1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Claim Secure English garage keepers lien florida tallahassee form |
SPECIAL AUTHORIZATION REQUEST
Fax Requests to
OR Mail Requests to Clinical Services, ClaimSecure Inc., Suite 620, 1 City Centre Drive, Mississauga, Ontario, L5B 1M2
PLEASE SUBMIT A COPY OF YOUR PHARMACY MEDICATION HISTORY FROM LAST YEAR.
Member Name
Patient Name
City
|
|
Group Number |
|
Certificate Number (10 Digits) |
|
|
|
|
|
|
|
Relationship to Member |
Address |
|
|||
Member |
Spouse Child Other |
|
|
|
|
Province |
|
Postal Code |
Telephone Number |
Patient Date of Birth (YYYY/MM/DD) |
|
( )
I hereby authorize any physician, hospital, insurance company, other healthcare professional and ClaimSecure to exchange information in connection with this claim for the purpose of special authorization/patient exception evaluation, adjudication of claims, and administration of my health benefit program. I assume responsibility for any cost required for the completion of this form. A photocopy of this authorization shall be as valid as the original.
Signature
X
TO BE COMPLETED BY PHYSICIAN ONLY (PLEASE PRINT CLEARLY)
Physician Name
Specialty Qualification
Address
City
Province
Postal Code
Physician Signature
X
Telephone Number
( |
) |
( |
) |
DRUG REQUESTED FOR SPECIAL AUTHORIZATION (1 FORM PER DRUG)
Drug Name |
Strength |
Diagnosis |
|
|
Sig
Duration of Therapy
PREVIOUS DRUGS PRESCRIBED FOR THIS CONDITION (IF APPLICABLE)
Drug Name
Reason for Discontinuation
Drug Name
Reason for Discontinuation
Strength |
Sig |
|
|
|
Duration of Therapy |
Strength |
Sig |
|
|
|
Duration of Therapy |
|
|
REASON FOR PRESCRIBING REQUESTED DRUG:
No other therapeutic alternative for patient’s medical condition
Prior therapy used was not effective: _______________________________________________________________________________________________
Could not tolerate prior therapy / side effects: ________________________________________________________________________________________
Other
(Please provide explanation below, or on the back of the form, to expand on checked item(s). Attach supporting documentation where applicable.)
RELEVANT MEDICAL INFORMATION (IF APPLICABLE): |
|
|
VIRAL GENOTYPE__________________ |
EDSS RATING___________________ |
WHO FUNCTIONAL CLASS_______________________ |
BASDAI/BASFI SCORE______________ |
HAQ DISABILITY INDEX__________ |
ECOG PERFORMANCE STATUS___________________ |
LAB RESULTS:___________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________
SITE OF DRUG ADMINISTRATION (IF APPLICABLE): |
|
|
|
||
Home |
Doctor’s Office |
Private Clinic |
Hospital Clinic |
Hospital |
LTC Facility |
INCOMPLETE FORMS WILL DELAY PROCESSING