
Using the online PDF editor by FormsPal, you'll be able to complete or modify sp66 form here. The editor is continually upgraded by our staff, receiving handy functions and becoming better. To get the ball rolling, take these easy steps:
Step 1: Just hit the "Get Form Button" at the top of this webpage to see our pdf file editing tool. Here you will find all that is necessary to work with your file.
Step 2: This editor provides you with the capability to work with the majority of PDF forms in many different ways. Enhance it by including any text, correct original content, and place in a signature - all within several clicks!
This PDF form will require some specific information; to ensure correctness, please take note of the recommendations just below:
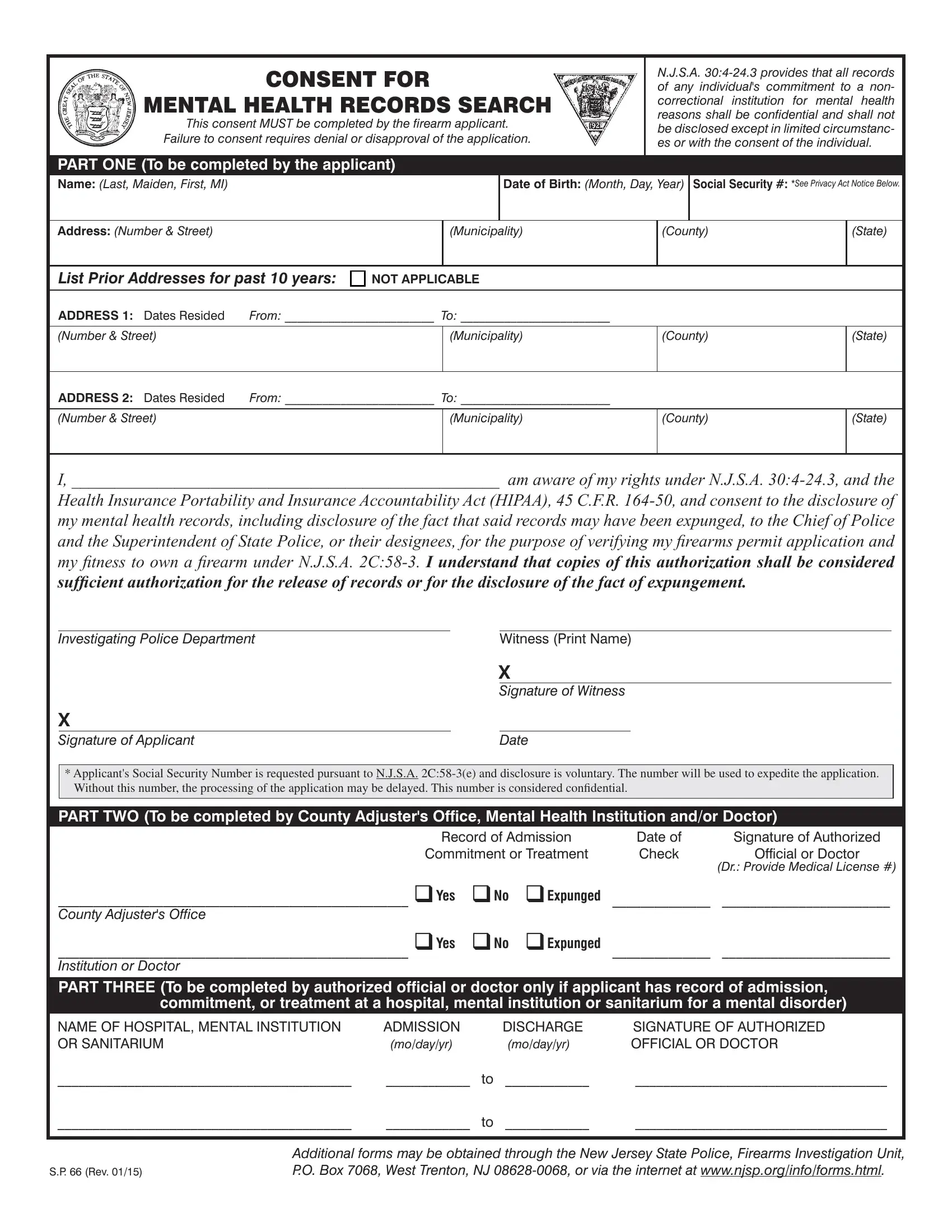
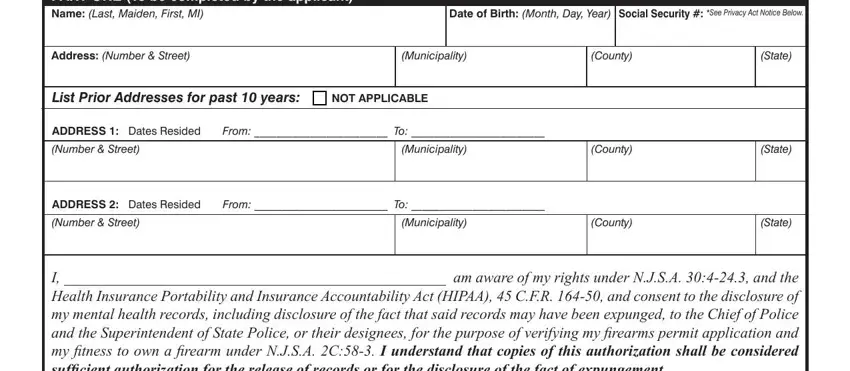
1. Begin completing your sp66 form with a number of essential blanks. Consider all the necessary information and be sure absolutely nothing is overlooked!
2. Soon after this selection of blank fields is done, proceed to type in the relevant information in these - I am aware of my rights under, Investigating Police Department, X Signature of Applicant, Witness Print Name, X Signature of Witness, Date, Applicants Social Security Number, Without this number the processing, PART TWO To be completed by County, County Adjusters Office, Record of Admission, Commitment or Treatment, Date of Check, Signature of Authorized, and Official or Doctor.
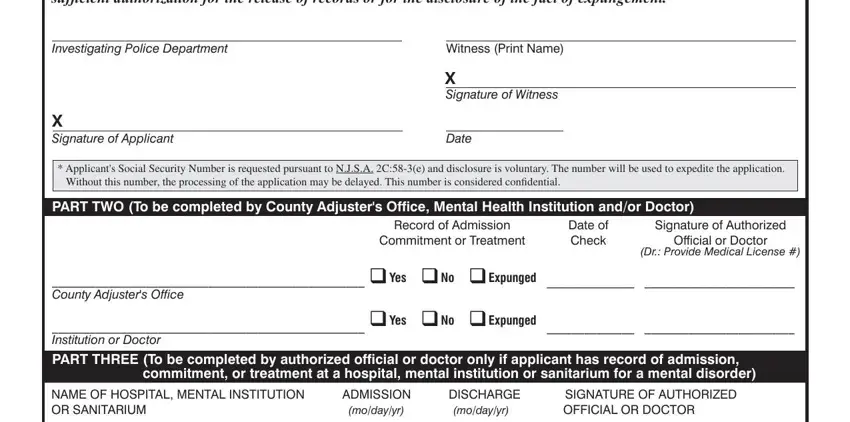
People often make errors when filling out Date of Check in this area. You should revise everything you type in here.
Step 3: Soon after rereading your fields and details, press "Done" and you're good to go! Try a free trial account at FormsPal and gain instant access to sp66 form - which you may then make use of as you wish inside your FormsPal cabinet. FormsPal ensures your information confidentiality by using a secure method that in no way saves or shares any private data used in the file. Feel safe knowing your files are kept safe every time you work with our tools!