
A client sheet information form is the foundation of efficient client onboarding and tax preparation. Follow the steps below to complete and use this document accurately.
How to Fill Out the Client Sheet Information Form
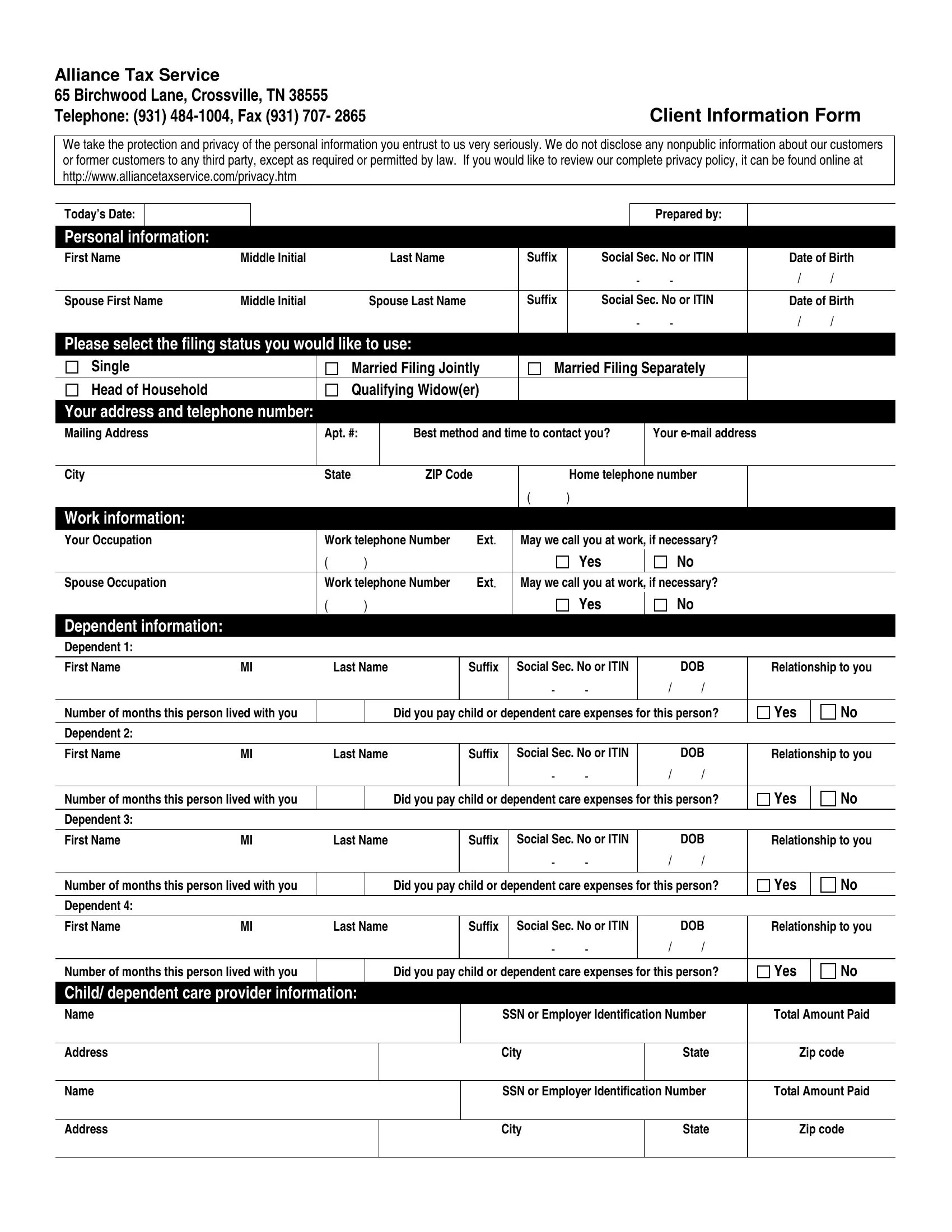
- Enter personal details: Provide your full legal name, date of birth, Social Security number, and any applicable suffix (Jr., Sr.).
- Add contact information: Include your home address, primary phone number with extension, and email address.
- List income sources: Record all wages, self-employment income, and investment accounts including Individual Retirement Accounts (IRAs).
- Include dependent data: List each qualifying dependent's full name, relationship, and Social Security number.
- Detail eligible deductions: Document alimony payments, unreimbursed medical expenses, charitable donations, and other deductible items.
- Review and submit: Confirm all entries are accurate before submitting to Alliance Tax Service at 65 Birchwood Lane, Crossville, TN.
Who Uses a Client Information Form?
Client information forms are used across tax preparation services, accounting firms, financial advisory practices, and legal offices. They help professionals centralize client data, ensure regulatory compliance, and streamline new client onboarding. Related documents include the new client data sheet and the client tax organizer.
What Is a Client Sheet Information Form Used For?
Tax preparers use client information forms to gather every data point needed for an accurate return, from personal identifiers to eligible deductions. By collecting this data upfront, firms like Alliance Tax Service minimize errors, protect client confidentiality, and maximize allowable returns. For additional intake documents, see the client intake form or the lawyer client intake form.
Privacy and Confidentiality
All data collected on a client sheet information form is treated as nonpublic personal information. Alliance Tax Service adheres to applicable federal and state privacy laws, sharing client details only as required by law or with explicit client consent.