
Handling PDF documents online is a piece of cake with our PDF editor. Anyone can fill in clinical review report form here with no trouble. To make our tool better and easier to work with, we constantly come up with new features, with our users' suggestions in mind. Starting is simple! All you should do is stick to the next basic steps down below:
Step 1: First of all, access the pdf tool by pressing the "Get Form Button" at the top of this page.
Step 2: The editor will let you work with PDF forms in many different ways. Enhance it by adding any text, correct what's already in the document, and place in a signature - all within a couple of mouse clicks!
Filling out this document demands thoroughness. Ensure that each field is filled in correctly.
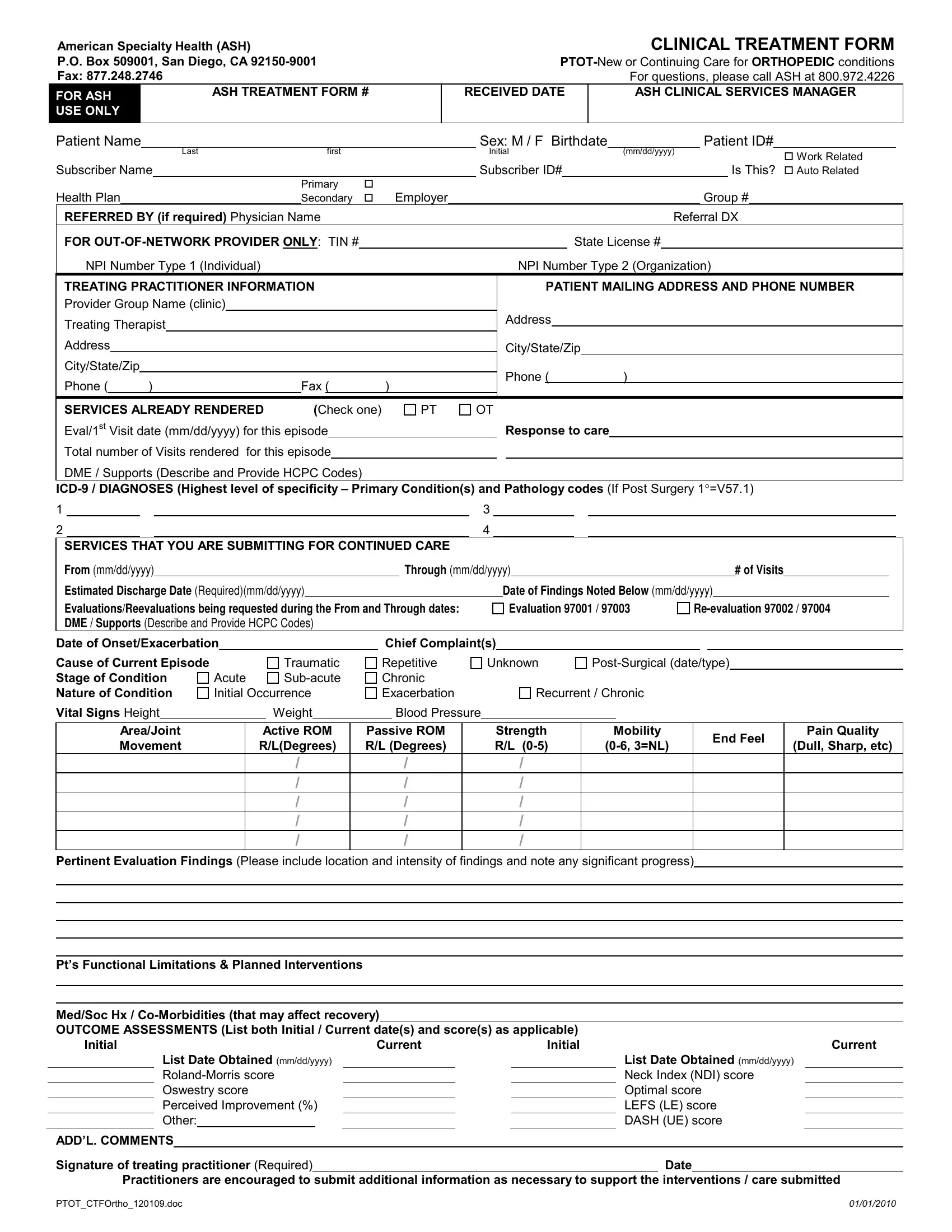
1. The clinical review report form involves certain information to be inserted. Make sure the next blanks are filled out:
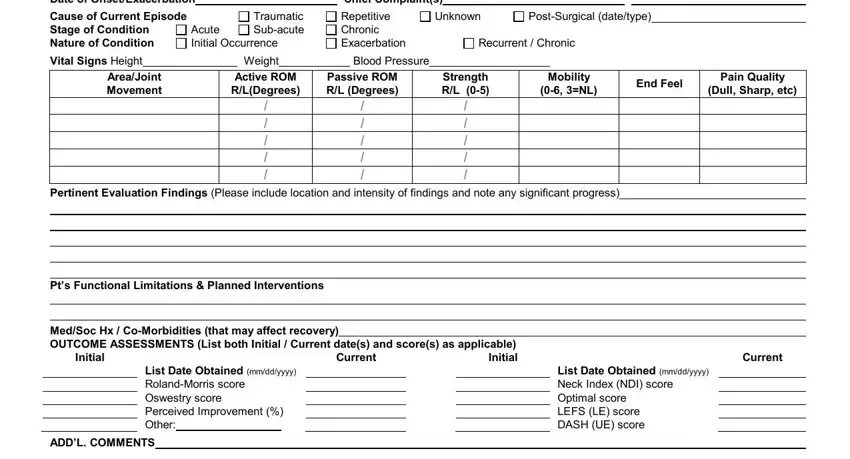
2. After filling out the previous step, go on to the next step and complete the necessary details in these fields - Date of OnsetExacerbation, Chief Complaints, Cause of Current Episode Stage of, Traumatic Subacute, Acute Initial Occurrence, Repetitive Chronic Exacerbation, Unknown, PostSurgical datetype, Recurrent Chronic, Vital Signs Height, Weight, Blood Pressure, AreaJoint Movement, Active ROM RLDegrees, and Passive ROM RL Degrees.
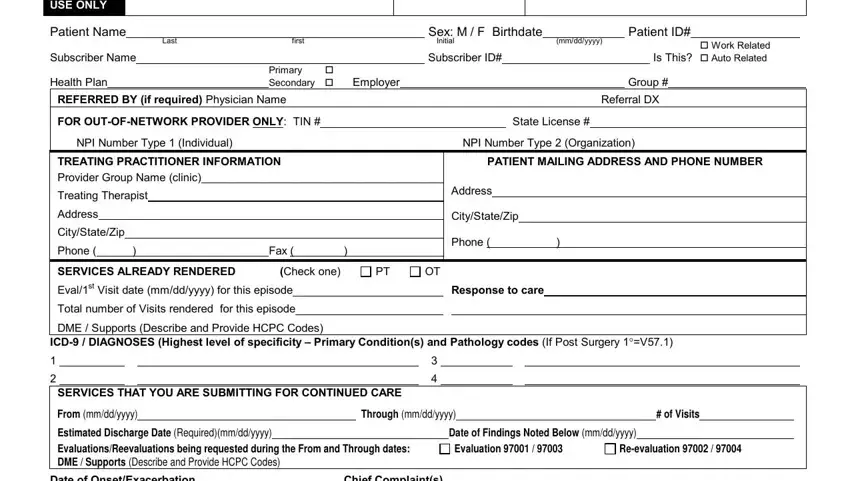
3. This third part is considered pretty straightforward, American Specialty Health ASH PO, Patient Name, Subscriber Name Health Plan, Last First Initial, Primary Secondary Employer, REFERRED BY if required Physician, Sex M F Birthdate, mmddyyyy, Subscriber ID, Patient ID, Work Related Is This Auto Related, Group, Referral DX, FOR OUTOFNETWORK PROVIDER ONLY TIN, and State License - all these empty fields must be filled out here.
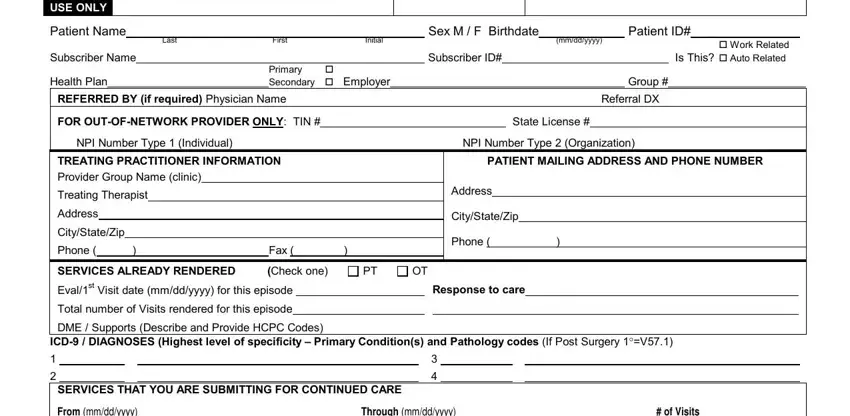
4. To go onward, this fourth step will require typing in a couple of form blanks. These include From mmddyyyy, Through mmddyyyy, of Visits, Estimated Discharge Date, Date of Findings Noted Below, Evaluation, Reevaluation, Date of Onset Exacerbation Cause, Vital Signs Height Cognitive, Traumatic, Congenital, Chief Complaints Unknown, PostSurgical DateType, Acute Initial Occurrence, and SubAcute, which are vital to continuing with this process.
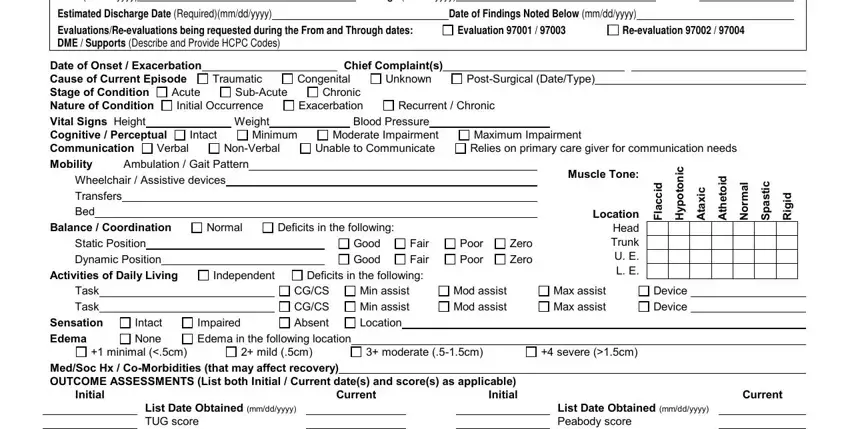
When it comes to Congenital and Date of Onset Exacerbation Cause, make sure that you don't make any mistakes here. These are the key ones in the page.
5. As you approach the completion of this document, you'll notice a few more requirements that need to be met. In particular, List Date Obtained mmddyyyy TUG, List Date Obtained mmddyyyy, ADDL COMMENTS, Signature of treating practitioner, Date, Practitioners are encouraged to, and PTOTCTFNeurodoc should be done.

Step 3: Spell-check all the information you have entered into the form fields and click on the "Done" button. Right after starting a7-day free trial account with us, you'll be able to download clinical review report form or email it without delay. The PDF document will also be accessible through your personal account menu with all your edits. FormsPal guarantees safe form tools without personal information recording or any sort of sharing. Rest assured that your data is secure with us!