

restriction of rights form can be filled in online without any problem. Simply make use of FormsPal PDF tool to finish the job quickly. To maintain our tool on the cutting edge of convenience, we aim to put into practice user-driven capabilities and improvements on a regular basis. We are routinely grateful for any suggestions - join us in remolding PDF editing. For anyone who is seeking to get started, here is what it takes:
Step 1: Open the PDF in our tool by pressing the "Get Form Button" at the top of this page.
Step 2: The tool allows you to customize almost all PDF forms in many different ways. Modify it with any text, adjust what is already in the PDF, and place in a signature - all close at hand!
This form will need some specific details; to guarantee accuracy and reliability, don't hesitate to take into account the suggestions down below:
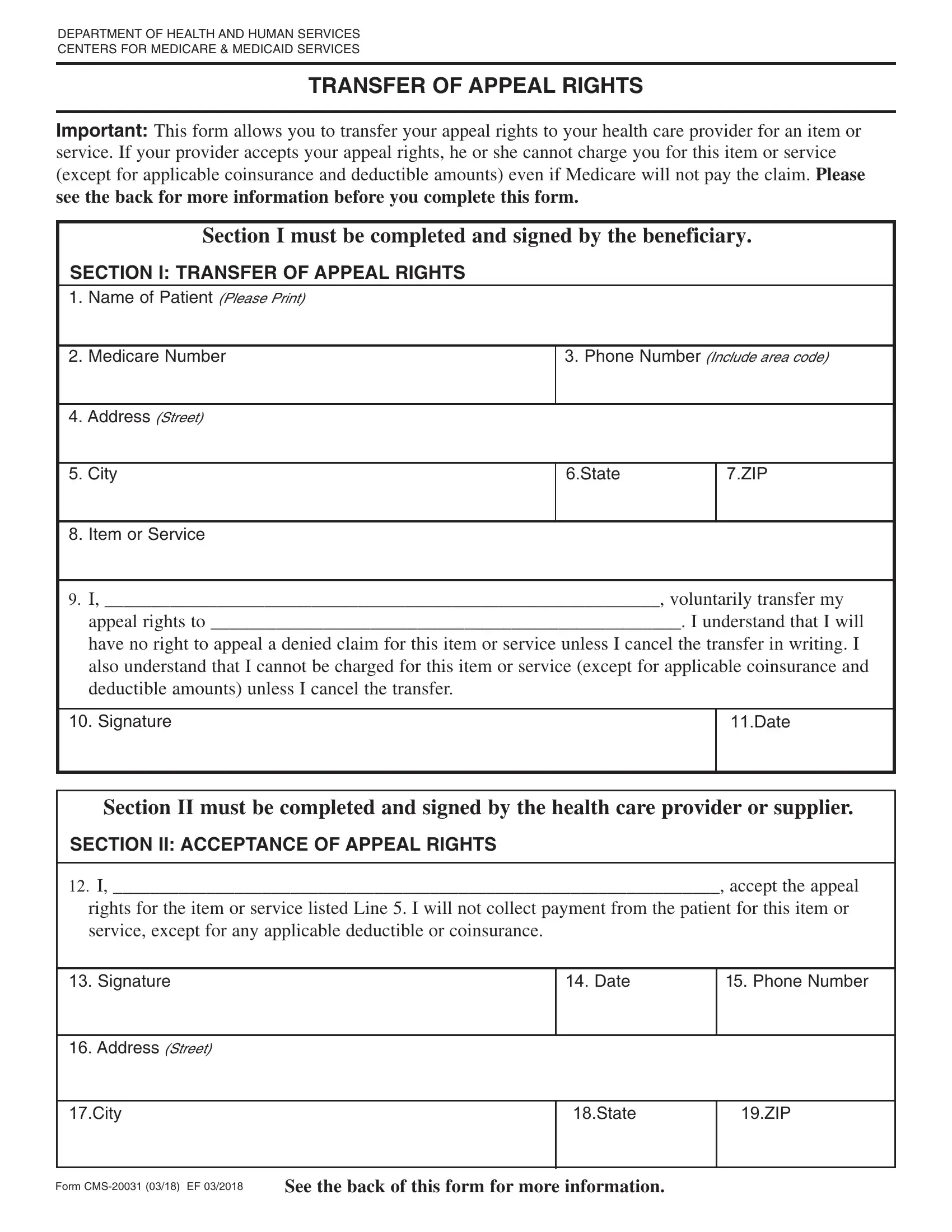
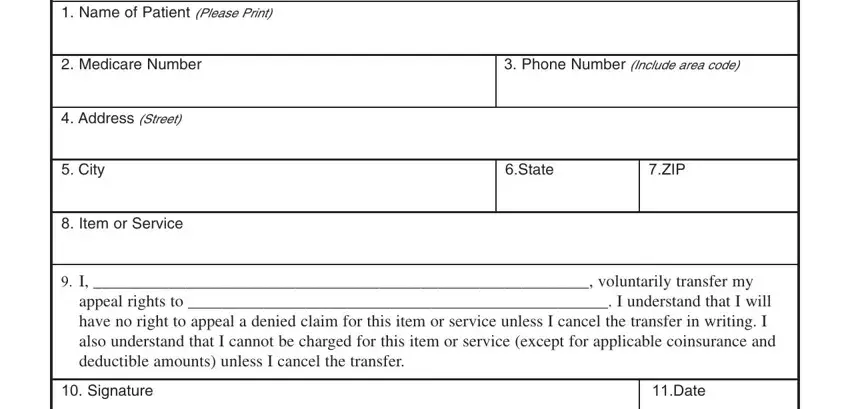
1. The restriction of rights form requires specific details to be inserted. Make certain the following fields are finalized:
2. Given that the previous array of fields is completed, it is time to include the necessary details in SECTION II ACCEPTANCE OF APPEAL, I accept the appeal rights for, Signature, Address Street, City, Date, Phone Number, State, ZIP, Form CMS EF, and See the back of this form for more so you're able to proceed to the 3rd stage.
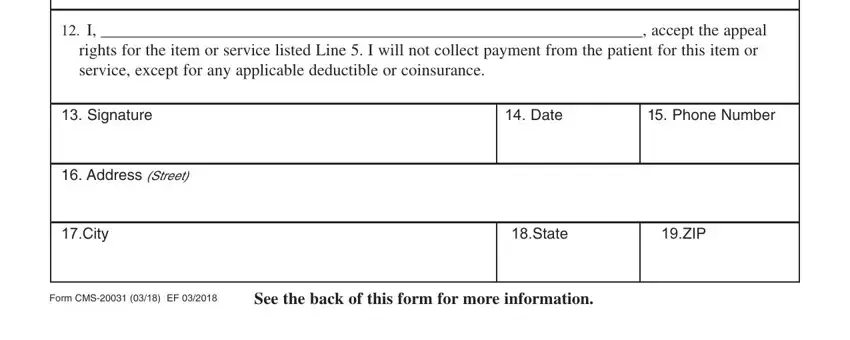
Concerning I accept the appeal rights for and City, be sure that you double-check them in this section. Those two are surely the most significant fields in this form.
Step 3: Just after taking one more look at your entries, click "Done" and you are all set! Join us right now and immediately get restriction of rights form, set for download. Every single change you make is handily saved , which means you can modify the document at a later time as required. FormsPal is focused on the privacy of our users; we make certain that all personal information handled by our editor is kept protected.