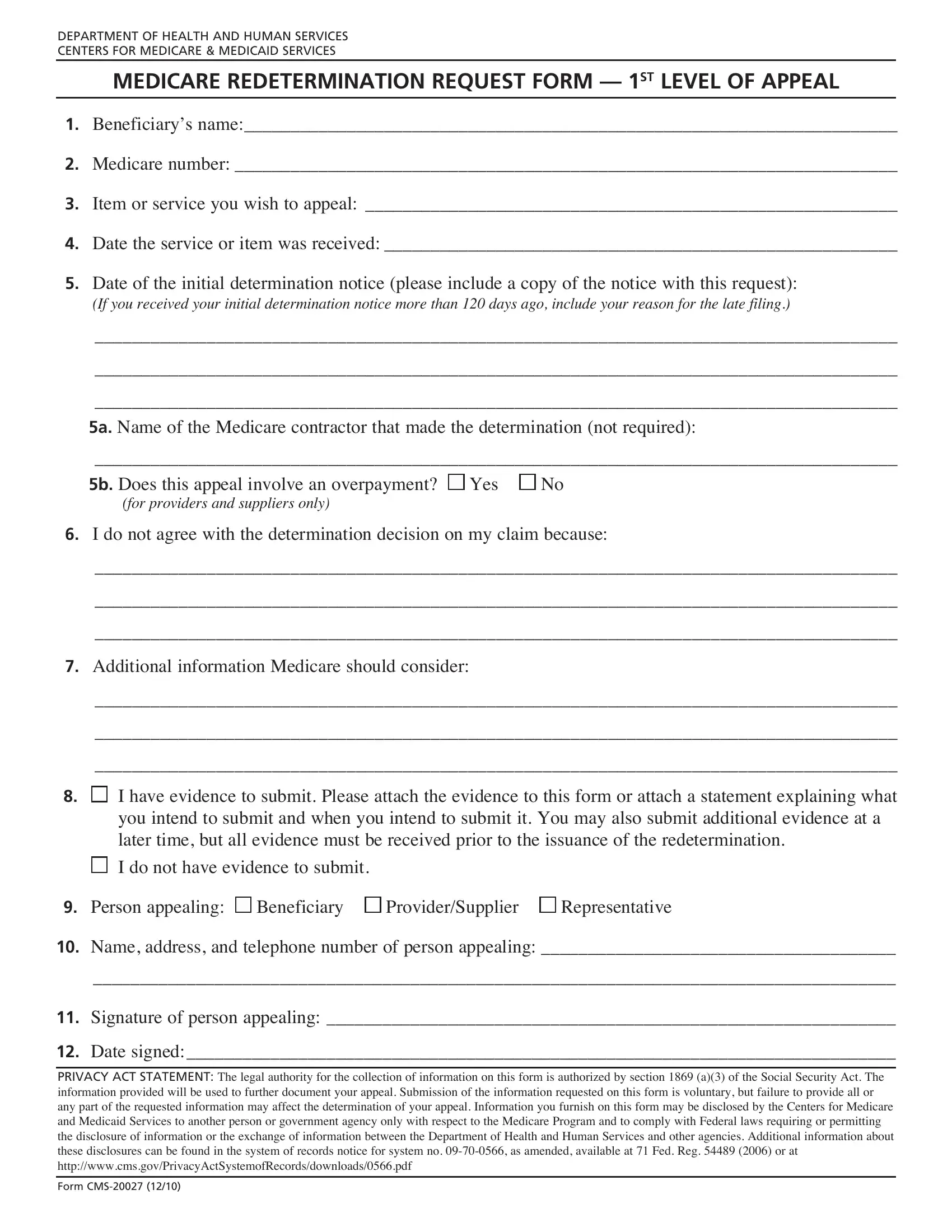
Navigating the Medicare system can often feel like a daunting endeavor, especially when it comes to disputing coverage decisions. For individuals or providers dissatisfied with a Medicare determination, the CMS 20027 form serves as a vital tool, enabling a formal request for reconsideration or the first level of appeal. This form, issued by the Department of Health and Human Services and managed by the Centers for Medicare & Medicaid Services, is designed to ensure that beneficiaries and providers have a clear and structured pathway to challenge decisions regarding item or service coverage. It requires detailed information such as the beneficiary’s name, Medicare number, the specific item or service under dispute, and the initial determination notice, among other critical pieces of evidence to support the appeal. Moreover, it includes sections to articulate the disagreement with the original decision and to submit any additional information that could influence the redetermination. The process for submitting this form is backed by legal mandates under the Social Security Act, emphasizing its significance in the Medicare appeal process. Failure to provide comprehensive documentation or adhering to the guidelines can impact the success of the appeal, underscoring the form's importance in safeguarding the rights of Medicare recipients and providers. Notably, this form also highlights stipulations for privacy and the lawful use of submitted information, ensuring that appellants’ details are handled with the utmost care and confidentiality, solely in the interest of resolving the appeal in accordance with federal regulations.
| Question | Answer |
|---|---|
| Form Name | Form Cms 20027 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cms, form cms 20027, pdf, 20037 |