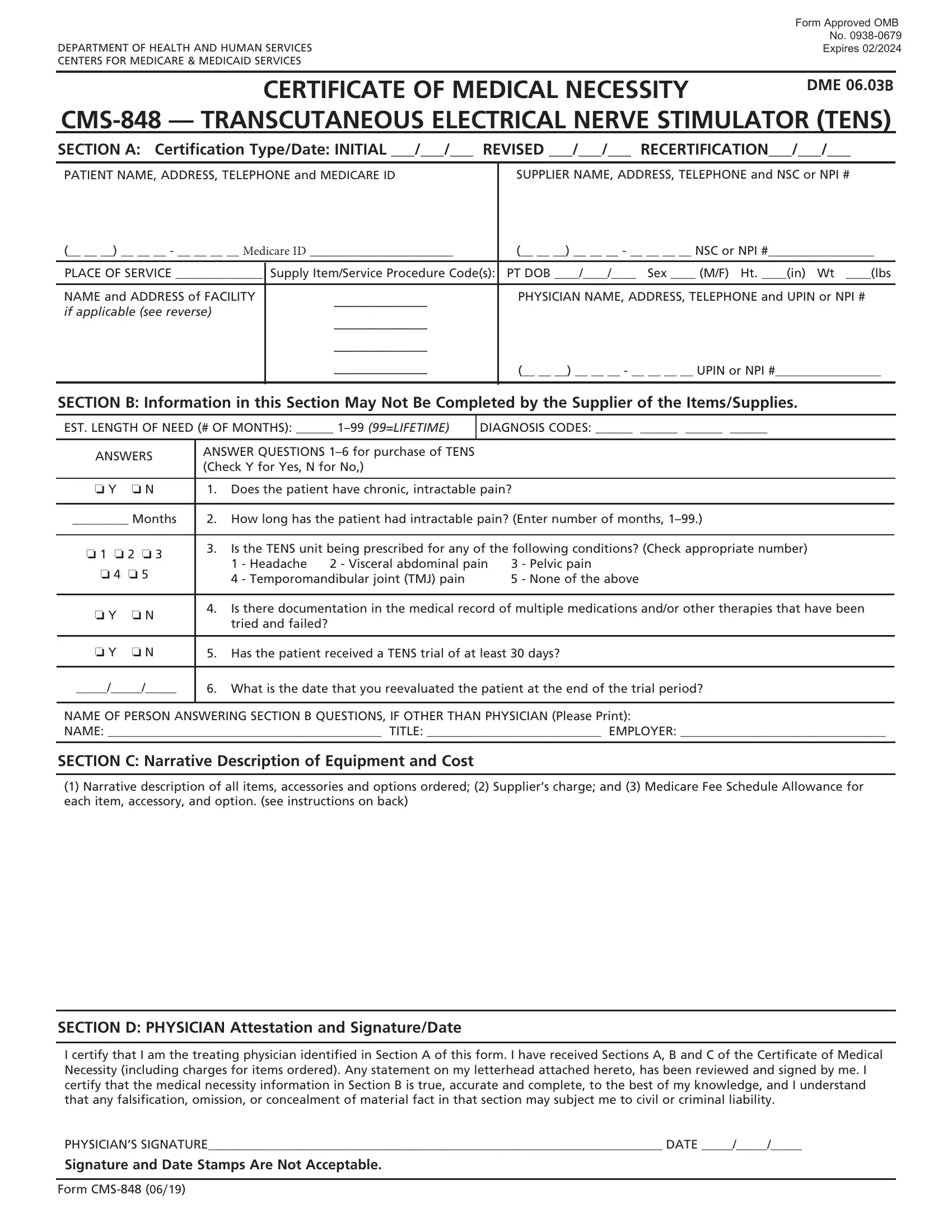
Understanding the complexities and requirements of healthcare documentation is crucial for patients seeking coverage for essential medical equipment. The CMS-848 form, a Certificate of Medical Necessity for a Transcutaneous Electrical Nerve Stimulator (TENS), serves as a pivotal piece of documentation within the Centers for Medicare & Medicaid Services. As part of the Department of Health and Human Services, this form, approved under OMB No. 0938-0679 and valid through February 2024, is designed to validate the necessity of a TENS device for individuals with chronic, intractable pain. It requires detailed information, including patient and supplier identification, the estimated length of need, diagnosis codes, and a detailed description of the equipment and cost. Furthermore, the CMS-848 form incorporates a section for the treating physician’s attestation to the medical necessity of the equipment, underscoring the importance of medical professional validation in the approval process. By scrutinizing several key areas, including patient eligibility, treatment history, and physician endorsement, this form plays a critical role in ensuring that Medicare beneficiaries receive the pain management solutions they require, adhering to stringent guidelines to combat misuse and ensure appropriate medical supervision.
| Question | Answer |
|---|---|
| Form Name | Cms 848 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cms 848, medical necessity completed, form 848 form, 848 necessity |
|
Form Approved OMB |
|
|
No. |
|
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
Expires 02/2024 |
|
CENTERS FOR MEDICARE & MEDICAID SERVICES |
|
|
|
|
|
CERTIFICATE OF MEDICAL NECESSITY |
DME 06.03B |
|
|
|
|
SECTION A: Certification Type/Date: INITIAL ___/___/___ |
REVISED ___/___/___ RECERTIFICATION___/___/___ |
|
|
PATIENT NAME, ADDRESS, TELEPHONE and MEDICARE ID |
SUPPLIER NAME, ADDRESS, TELEPHONE and NSC or NPI # |
(__ __ __) __ __ __ - __ __ __ __ Medicare ID _______________________ |
(__ __ __) __ __ __ - __ __ __ __ NSC or NPI #_________________ |
|
PLACE OF SERVICE ______________ |
Supply Item/Service Procedure Code(s): |
PT DOB ____/____/____ Sex ____ (M/F) Ht. ____(in) Wt ____(lbs |
|
|
|
NAME and ADDRESS of FACILITY |
__________ |
PHYSICIAN NAME, ADDRESS, TELEPHONE and UPIN or NPI # |
if applicable (see reverse) |
__________ |
|
|
|
|
|
__________ |
|
|
__________ |
(__ __ __) __ __ __ - __ __ __ __ UPIN or NPI #_________________ |
|
|
|
SECTION B: Information in this Section May Not Be Completed by the Supplier of the Items/Supplies.
EST. LENGTH OF NEED (# OF MONTHS): ______
DIAGNOSIS CODES: ______ ______ ______ ______
ANSWERS |
ANSWER QUESTIONS |
|
|||
(Check Y for Yes, N for No,) |
|
||||
|
|
|
|||
|
|
|
|
||
o Y |
o N |
1. |
Does the patient have chronic, intractable pain? |
||
|
|
|
|||
_________ Months |
2. |
How long has the patient had intractable pain? (Enter number of months, |
|||
|
|
|
|
||
o 1 o 2 o 3 |
3. |
Is the TENS unit being prescribed for any of the following conditions? (Check appropriate number) |
|||
|
1 - Headache |
2 - Visceral abdominal pain |
3 - Pelvic pain |
||
o 4 o 5 |
|
||||
|
4 - Temporomandibular joint (TMJ) pain |
5 - None of the above |
|||
|
|
|
|||
|
|
|
|
||
o Y |
o N |
4. |
Is there documentation in the medical record of multiple medications and/or other therapies that have been |
||
|
tried and failed? |
|
|
||
|
|
|
|
|
|
|
|
|
|
||
o Y |
o N |
5. |
Has the patient received a TENS trial of at least 30 days? |
||
_____/_____/_____
6.What is the date that you reevaluated the patient at the end of the trial period?
NAME OF PERSON ANSWERING SECTION B QUESTIONS, IF OTHER THAN PHYSICIAN (Please Print):
NAME: ____________________________________________ TITLE: ____________________________ EMPLOYER: _________________________________
SECTION C: Narrative Description of Equipment and Cost
(1)Narrative description of all items, accessories and options ordered; (2) Supplier’s charge; and (3) Medicare Fee Schedule Allowance for each item, accessory, and option. (see instructions on back)
SECTION D: PHYSICIAN Attestation and Signature/Date
I certify that I am the treating physician identified in Section A of this form. I have received Sections A, B and C of the Certificate of Medical Necessity (including charges for items ordered). Any statement on my letterhead attached hereto, has been reviewed and signed by me. I certify that the medical necessity information in Section B is true, accurate and complete, to the best of my knowledge, and I understand that any falsification, omission, or concealment of material fact in that section may subject me to civil or criminal liability.
PHYSICIAN’S SIGNATURE_________________________________________________________________________ DATE _____/_____/_____
Signature and Date Stamps Are Not Acceptable.
Form

INSTRUCTIONS FOR COMPLETING THE CERTIFICATE OF MEDICAL NECESSITY FOR TRANSCUTANEOUS ELECTRICAL NERVE STIMULATOR (TENS)
SECTION A: |
(May be completed by the supplier) |
CERTIFICATION |
If this is an initial certification for this patient, indicate this by placing date (MM/DD/YY) needed initially in the space |
TYPE/DATE: |
marked “INITIAL.” If this is a revised certification (to be completed when the physician changes the order, based on the |
|
patient’s changing clinical needs), indicate the initial date needed in the space marked “INITIAL,” and indicate the |
|
recertification date in the space marked “REVISED.” If this is a recertification, indicate the initial date needed in the |
|
space marked “INITIAL,” and indicate the recertification date in the space marked “RECERTIFICATION.” Whether |
|
submitting a REVISED or a RECERTIFIED CMN, be sure to always furnish the INITIAL date as well as the REVISED or |
|
RECERTIFICATION date. |
PATIENT |
Indicate the patient’s name, permanent legal address, telephone number and his/her Medicare ID as it appears on his/her |
INFORMATION: |
Medicare card and on the claim form. |
SUPPLIER |
Indicate the name of your company (supplier name), address and telephone number along with the Medicare Supplier |
INFORMATION: |
Number assigned to you by the National Supplier Clearinghouse (NSC) or applicable National Provider Identifier (NPI). If |
|
using the NPI Number, indicate this by using the qualifier XX followed by the |
|
e.g. NSC number, use the qualifier 1C followed by the |
PLACE OF SERVICE: |
Indicate the place in which the item is being used, i.e., patient’s home is 12, skilled nursing facility (SNF) is 31, End |
|
Stage Renal Disease (ESRD) facility is 65, etc. Refer to the DMERC supplier manual for a complete list. |
FACILITY NAME: |
If the place of service is a facility, indicate the name and complete address of the facility. |
SUPPLY ITEM/SERVICE |
List all procedure codes for items ordered. Procedure codes that do not require certification should not be listed |
PROCEDURE CODE(S): |
on the CMN. |
PATIENT DOB, HEIGHT, |
Indicate patient’s date of birth (MM/DD/YY) and sex (male or female); height in inches and weight in pounds, if requested. |
WEIGHT AND SEX: |
|
PHYSICIAN NAME, |
Indicate the PHYSICIAN’S name and complete mailing address. |
ADDRESS: |
|
PHYSICIAN |
Accurately indicate the treating physician’s Unique Physician Identification Number (UPIN) or applicable National |
INFORMATION: |
Provider Identifier (NPI). If using the NPI Number, indicate this by using the qualifier XX followed by the |
|
If using UPIN number, use the qualifier 1G followed by the |
PHYSICIAN’S |
Indicate the telephone number where the physician can be contacted (preferably where records would be accessible |
TELEPHONE NO: |
pertaining to this patient) if more information is needed. |
SECTION B: |
(May not be completed by the supplier. While this section may be completed by a |
|
Physician employee, it must be reviewed, and the CMN signed (in Section D) by the treating practitioner.) |
EST. LENGTH OF NEED: |
Indicate the estimated length of need (the length of time the physician expects the patient to require use of the ordered |
|
item) by filling in the appropriate number of months. If the patient will require the item for the duration of his/her life, |
|
then enter “99”. |
DIAGNOSIS CODES: |
In the first space, list the diagnosis code that represents the primary reason for ordering this item. List any additional |
|
diagnosis codes that would further describe the medical need for the item (up to 4 codes). |
QUESTION SECTION: |
This section is used to gather clinical information to help Medicare determine the medical necessity for the item(s) |
|
being ordered. Answer each question which applies to the items ordered, checking “Y” for yes, “N” for no, or “D” for |
|
does not apply. |
NAME OF PERSON |
If a clinical professional other than the treating physician (e.g., home health nurse, physical therapist, dietician) or a |
ANSWERING SECTION B |
physician employee answers the questions of Section B, he/she must print his/her name, give his/her professional title |
QUESTIONS: |
and the name of his/her employer where indicated. If the physician is answering the questions, this space may be left blank. |
SECTION C: |
(To be completed by the supplier) |
NARRATIVE |
Supplier gives (1) a narrative description of the item(s) ordered, as well as all options, accessories, supplies and drugs; |
DESCRIPTION OF |
(2) the supplier’s charge for each item(s), options, accessories, supplies and drugs; and (3) the Medicare fee schedule |
EQUIPMENT & COST: |
allowance for each item(s), options, accessories, supplies and drugs, if applicable. |
SECTION D: |
(To be completed by the physician) |
PHYSICIAN |
The physician’s signature certifies (1) the CMN which he/she is reviewing includes Sections A, B, C and D; (2) the |
ATTESTATION: |
answers in Section B are correct; and (3) the |
PHYSICIAN SIGNATURE |
After completion and/or review by the physician of Sections A, B and C, the physician’s must sign and date the CMN in |
AND DATE: |
Section D, verifying the Attestation appearing in this Section. The physician’s signature also certifies the items ordered |
|
are medically necessary for this patient. |
According to According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
DO NOT SUBMIT CLAIMS TO THIS ADDRESS. Please see http://www.medicare.gov/ for information on claim filing.
Form