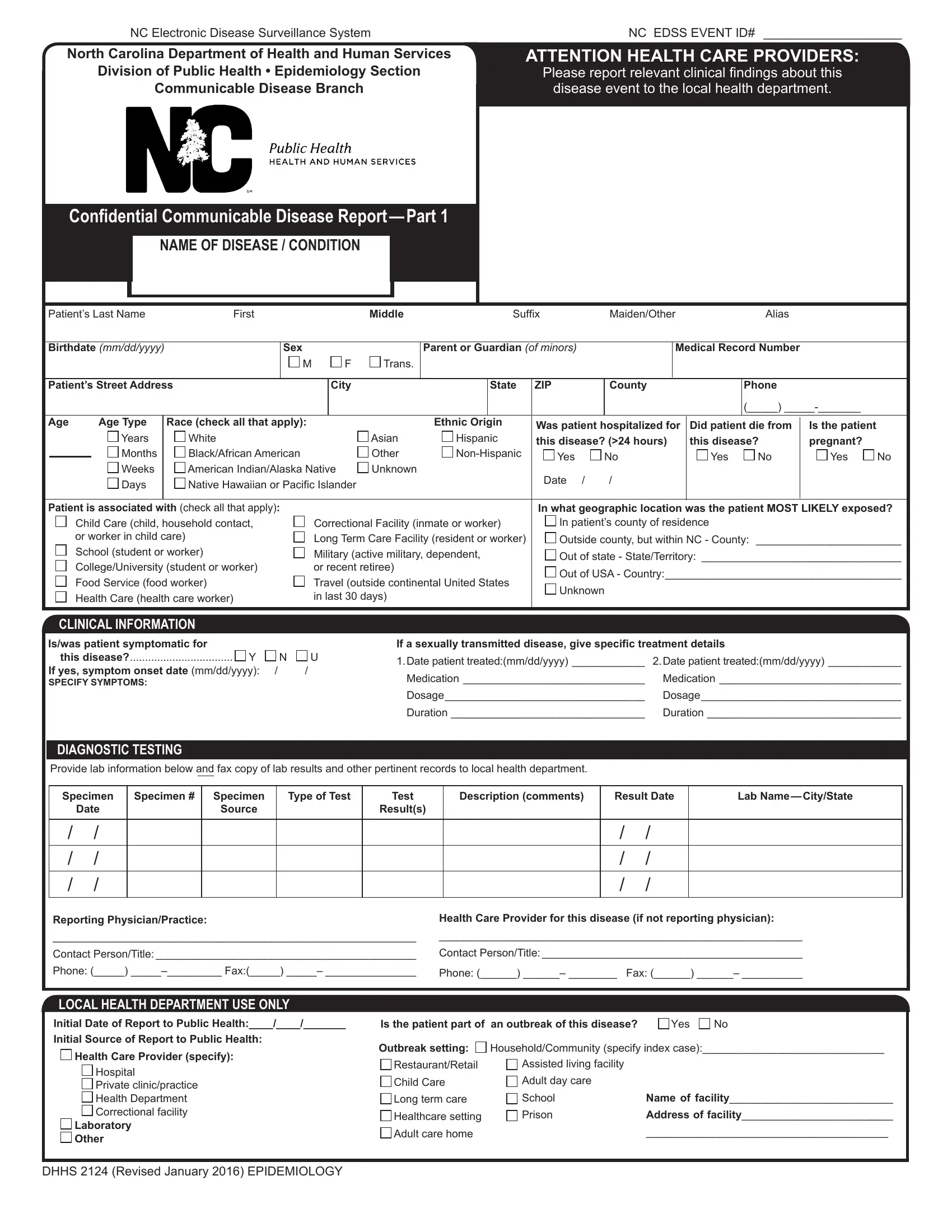
In the realm of public health and disease surveillance, the Confidential Communicable Disease Report Part 1 serves as an indispensable tool, especially within the North Carolina Electronic Disease Surveillance System (NC EDSS). This document, framed under the guidance of the North Carolina Department of Health and Human Services Division of Public Health and its Epidemiology Section, Communicable Disease Branch, undertakes the critical responsibility of cataloging and tracking disease occurrences across the state. Health care providers are called upon to relay pertinent clinical findings to local health departments, ensuring a prompt and coordinated response to health threats. The form covers extensive ground, requesting detailed patient information such as demographics, disease specifics, and clinical data including symptoms, diagnostic testing, and treatment details. Furthermore, it navigates through the patient's exposure settings, potentially linking individual cases to larger outbreak patterns. This tool not only aids in immediate public health responses but also builds a data-driven foundation for understanding disease dynamics, highlighting risks associated with specific locations or populations, and therefore guiding preventive strategies. Amid its rigorous adherence to privacy standards—precisely aligning with HIPAA Privacy Rule exemptions and North Carolina's state laws on communicable disease reporting—this form embodies a crucial balance between individual confidentiality and the collective right to health security.
| Question | Answer |
|---|---|
| Form Name | Communicable Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | disease form, communicable disease form, north carolina communiable disease form editable, nc communicable form |
NC Electronic Disease Surveillance System |
NC EDSS EVENT ID# ____________________ |
North Carolina Department of Health and Human Services
Division of Public Health • Epidemiology Section
Communicable Disease Branch
Confidential Communicable Disease Report — Part 1
NAME OF DISEASE / CONDITION
ATTENTION HEALTH CARE PROVIDERS:
Please report relevant clinical findings about this disease event to the local health department.
Patient’s Last Name |
First |
|
|
|
|
|
Middle |
|
|
Suffix |
Maiden/Other |
|
Alias |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birthdate (mm/dd/yyyy) |
|
|
Sex |
|
|
|
|
|
Parent or Guardian (of minors) |
|
|
Medical Record Number |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
M |
|
F |
Trans. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Patient’s Street Address |
|
|
|
|
City |
|
|
|
State |
ZIP |
County |
|
|
|
Phone |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(_____) |
|
|
Age |
|
Age Type |
|
Race (check all that apply): |
|
|
|
|
Ethnic Origin |
Was patient hospitalized for |
Did patient die from |
Is the patient |
|
||||||||||
|
|
|
|
Years |
|
White |
|
|
|
|
|
Asian |
|
Hispanic |
this disease? (>24 hours) |
this disease? |
pregnant? |
|
|||||
|
|
|
|
Months |
|
Black/African American |
|
|
|
Other |
|
Yes |
No |
|
|
Yes |
No |
Yes |
No |
||||
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
Weeks |
|
American Indian/Alaska Native |
Unknown |
Date / |
/ |
|
|
|
|
|
|
||||||||
|
|
|
|
Days |
|
Native Hawaiian or Pacific Islander |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Patient is associated with (check all that apply): |
|
|
|
|
|
|
|
In what geographic location was the patient MOST LIKELY exposed? |
|||||||||||||||
|
|
|
Child Care (child, household contact, |
|
|
|
Correctional Facility (inmate or worker) |
In patient’s county of residence |
|
|
|
||||||||||||
|
|
|
or worker in child care) |
|
|
|
Long Term Care Facility (resident or worker) |
Outside county, but within NC - County: ________________________ |
|||||||||||||||
|
|
|
School (student or worker) |
|
|
|
Military (active military, dependent, |
Out of state - State/Territory: _________________________________ |
|||||||||||||||
|
|
|
College/University (student or worker) |
|
|
|
or recent retiree) |
|
|
|
Out of USA - Country:_______________________________________ |
||||||||||||
|
|
|
Food Service (food worker) |
|
|
|
Travel (outside continental United States |
||||||||||||||||
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|||||||||||
|
|
|
Health Care (health care worker) |
|
|
|
in last 30 days) |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Is/was patient symptomatic for |
|
|
|
|
|
If a sexually transmitted disease, give specific treatment details |
|
|
|
||||||||||||||
|
|
this disease?.................................. Y |
N |
U |
1.Date patient treated:(mm/dd/yyyy) ____________ |
2.Date patient treated:(mm/dd/yyyy) ____________ |
|||||||||||||||||
If yes, symptom onset date (mm/dd/yyyy): |
/ |
|
/ |
|
|
|
Medication ______________________________ |
Medication ______________________________ |
|||||||||||||||
SPECIFY SYMPTOMS: |
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Dosage_________________________________ |
Dosage_________________________________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Duration ________________________________ |
Duration ________________________________ |
|||||||||
DIAGNOSTIC TESTING
Provide lab information below and fax copy of lab results and other pertinent records to local health department.
Specimen |
Specimen # |
Specimen |
Type of Test |
Test |
Description (comments) |
Result Date |
Lab |
||
|
Date |
|
Source |
|
Result(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
/ |
/ |
|
/ |
/ |
|
|
|
|
|
/ |
/ |
|
/ |
/ |
|
|
|
|
|
/ |
/ |
|
Reporting Physician/Practice:
____________________________________________________________
Contact Person/Title: ___________________________________________
Phone: (_____)
Health Care Provider for this disease (if not reporting physician):
____________________________________________________________
Contact Person/Title: ___________________________________________
Phone: (______) ______– ________ Fax: (______) ______– __________
LOCAL HEALTH DEPARTMENT USE ONLY
Initial Date of Report to Public Health:____/____/_______
Initial Source of Report to Public Health: Health Care Provider (specify):
Hospital
Private clinic/practice
Health Department
Correctional facility
Laboratory
Other
Is the patient part of |
an outbreak of this disease? |
Yes |
No |
Outbreak setting: |
Household/Community (specify index case):______________________________ |
||
Restaurant/Retail |
Assisted living facility |
|
|
Child Care |
Adult day care |
|
|
Long term care |
School |
Name of facility___________________________ |
|
Healthcare setting |
Prison |
Address of facility_________________________ |
|
Adult care home |
|
________________________________________ |
|
DHHS 2124 (Revised January 2016) EPIDEMIOLOGY
Diseases and Conditions Reportable in North Carolina
Physicians must report these diseases and conditions to the county local health department, according to the North Carolina Administrative Code: 10A NCAC 41A.0101 Reportable Diseases and Conditions (see below). Contact information for local health departments can be accessed at www.ncalhd.org/directors. If you are unable to contact your local health department, call the 24/7 pager for N.C. Communicable Disease Branch (919)
For diseases and conditions required to be reported within 24 hours, the initial report shall be made by telephone to the local health department, and the written disease report be made within 7 days. The reporting rules and disease report forms can be accessed at: http://epi.publichealth.nc.gov/cd/report.html
Diseases in BOLD ITALICS should be reported immediately to local health department.
Reportable to Local Health Department Within
DISEASE/CONDITION 24 Hours
ANTHRAX...............................................................................................
BOTULISM, FOODBORNE ....................................................................
BOTULISM, INTESTINAL (INFANT) ......................................................
BOTULISM, WOUND..............................................................................
Campylobacter infection..........................................................................
Chancroid ................................................................................................
Chikungunya ............................................................................................
Cholera ....................................................................................................
Cryptosporidiosis .....................................................................................
Cyclosporiasis .........................................................................................
Diphtheria ................................................................................................
E.coli infection, shiga
Foodborne disease: Clostridium perfringens...........................................
Foodborne: staphylococcal......................................................................
Foodborne disease: other/unknown ........................................................
Foodborne poisoning: ciguatera..............................................................
Foodborne poisoning: mushroom............................................................
Foodborne poisoning: scombroid fish......................................................
Gonorrhea ...............................................................................................
Granuloma inguinale ...............................................................................
Haemophilus influenzae,
invasive disease ....................................................................................
HEMORRHAGIC FEVER VIRUS
INFECTION .............................................................................................
Hepatitis A................................................................................................
Hepatitis B, acute ....................................................................................
HIV/AIDS
HIV.........................................................................................................
AIDS ......................................................................................................
Influenza virus infection causing death ....................................................
Listeriosis.................................................................................................
Measles (rubeola)....................................................................................
Meningococcal disease, invasive ............................................................
Middle East respiratory syndrome (MERS) .............................................
Monkeypox ..............................................................................................
NOVEL INFLUENZA VIRUS INFECTION...............................................
Ophthalmia neonatorum..........................................................................
Pertussis (Whooping Cough)...................................................................
PLAGUE..................................................................................................
Poliomyelitis, paralytic .............................................................................
Rabies, human ........................................................................................
Rubella ....................................................................................................
Salmonellosis ..........................................................................................
S. aureus with reduced susceptibility to vancomycin ..............................
SARS coronavirus infection ..................................................................
Shigellosis ...............................................................................................
SMALLPOX.............................................................................................
Syphilis
primary...................................................................................................
secondary..............................................................................................
early latent.............................................................................................
late latent...............................................................................................
late with clinical manifestations..............................................................
congenital ..............................................................................................
Tuberculosis ............................................................................................
TULAREMIA ...........................................................................................
Typhoid Fever, acute ...............................................................................
Vaccinia ...................................................................................................
Vibrio infection, other than cholera & vulnificus.......................................
Vibrio vulnificus .......................................................................................
Zika..........................................................................................................
DHHS 2124 (Revised January 2016) EPIDEMIOLOGY
Reportable to Local Health Department Within
DISEASE/CONDITION 7 Days
Brucellosis ................................................................................................
Chlamydial
Dengue .....................................................................................................
Ehrlichiosis, HGA (human granulocytic anaplasmosis) ............................
Ehrlichiosis, HME (human monocytic or e. chaffeensis) ..........................
Ehrlichiosis, unspecified ...........................................................................
Encephalitis, arboviral, WNV ....................................................................
Encephalitis, arboviral, LAC .....................................................................
Encephalitis, arboviral, EEE .....................................................................
Encephalitis, arboviral, other ....................................................................
Hantavirus infection..................................................................................
Hepatitis B, carriage .................................................................................
Hepatitis B, perinatally acquired...............................................................
Hepatitis C, acute .....................................................................................
Legionellosis.............................................................................................
Leprosy ....................................................................................................
Leptospirosis ............................................................................................
Lyme disease ...........................................................................................
Lymphogranuloma venereum...................................................................
Malaria......................................................................................................
Meningitis, pneumococcal ........................................................................
Mumps......................................................................................................
Pelvic inflammatory disease......................................................................
Psittacosis ................................................................................................
Q fever......................................................................................................
Rocky Mountain Spotted Fever ................................................................
Rubella, congenital syndrome ..................................................................
Streptococcal infection, Group A, invasive ...............................................
Tetanus .....................................................................................................
Toxic shock syndrome,
Toxic shock syndrome, streptococcal.......................................................
Trichinosis ................................................................................................
Typhoid, carriage (Salmonella typhi) ........................................................
Yellow fever ..............................................................................................
You may be contacted by the local health department for additional information about this case. Medical record information relevant to the investigation and/or control of a communicable disease is exempt from the HIPAA Privacy Rule (see 45 CFR 164.512(a) ) and is permitted as an exception to confidentiality of records in NC State Law GS § 130
North Carolina General Statute:
A physician licensed to practice medicine who has reason to suspect that a person about whom the physician has been consulted professionally has a
communicable disease or communicable condition declared by the : Commission to be reported, shall report information required by the Commission to the local health director of the county or district in which the physician is consulted.
North Carolina Administrative Code:
10A NCAC 41A.0101 Reportable Diseases and Conditions
(a)The following named diseases and conditions are declared to be dangerous to the public health and are hereby made reportable within the time period specified after the disease or condition is reasonably suspected to exist: