
dmv morbidity report can be filled in online with ease. Just try FormsPal PDF tool to complete the job quickly. To have our editor on the leading edge of convenience, we strive to put into operation user-driven capabilities and enhancements on a regular basis. We are always happy to receive feedback - play a vital role in revampimg PDF editing. With just a few easy steps, it is possible to begin your PDF editing:
Step 1: Click the orange "Get Form" button above. It is going to open up our pdf tool so you can begin filling out your form.
Step 2: After you start the PDF editor, you will notice the document made ready to be filled out. Aside from filling in various fields, it's also possible to perform many other things with the PDF, specifically adding any words, editing the original text, inserting illustrations or photos, signing the document, and more.
This document will need particular info to be entered, hence you must take the time to fill in precisely what is expected:
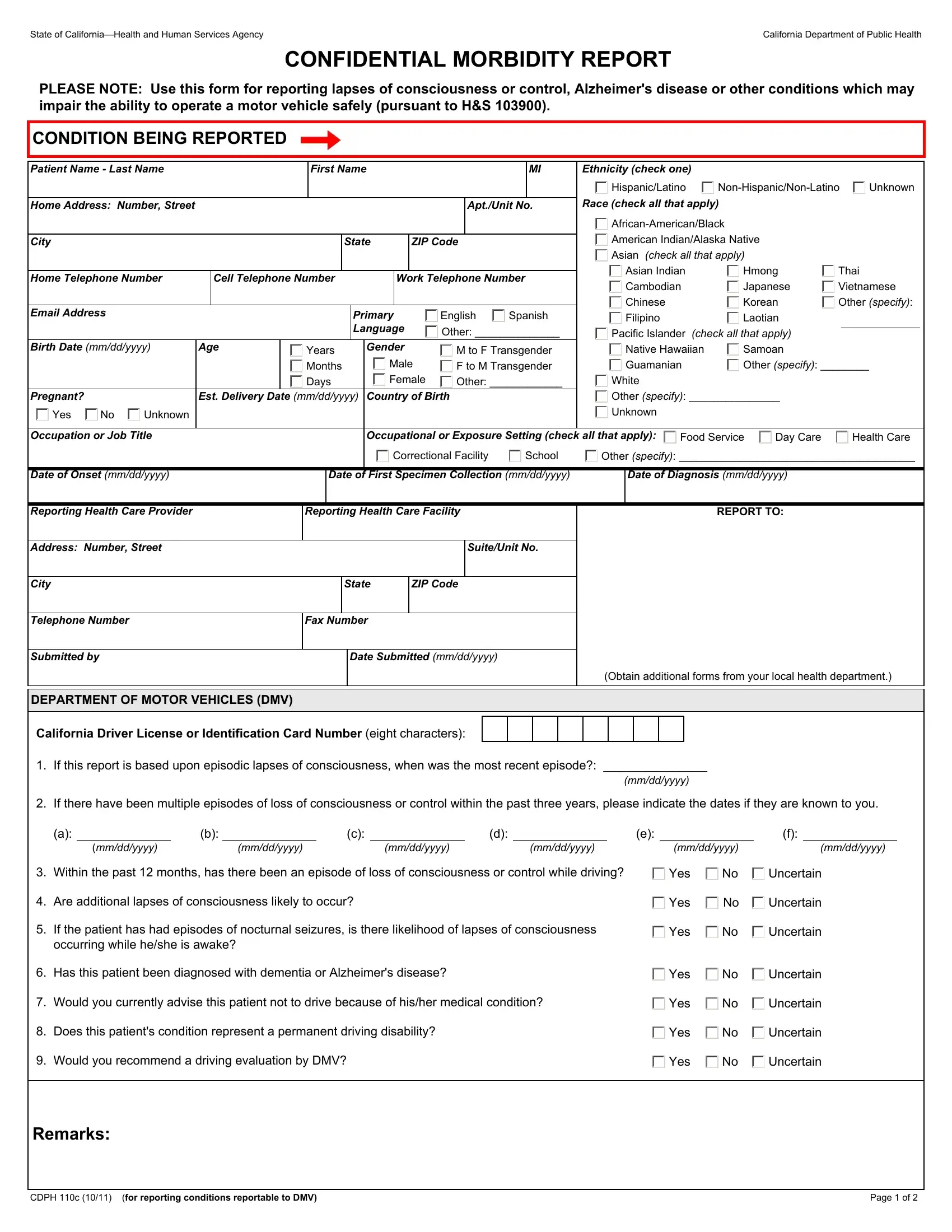
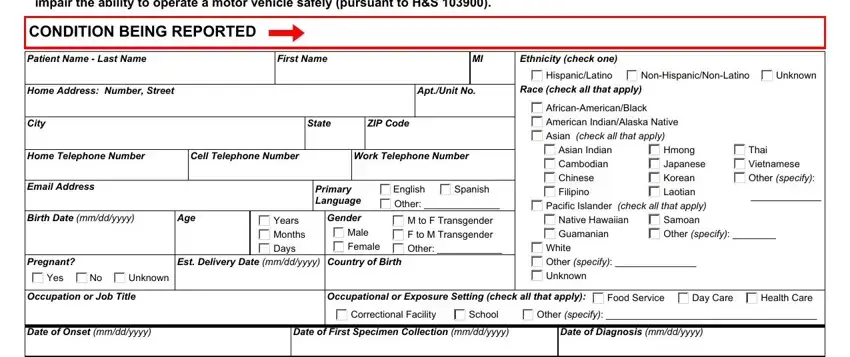
1. For starters, when filling in the dmv morbidity report, start in the part containing subsequent fields:
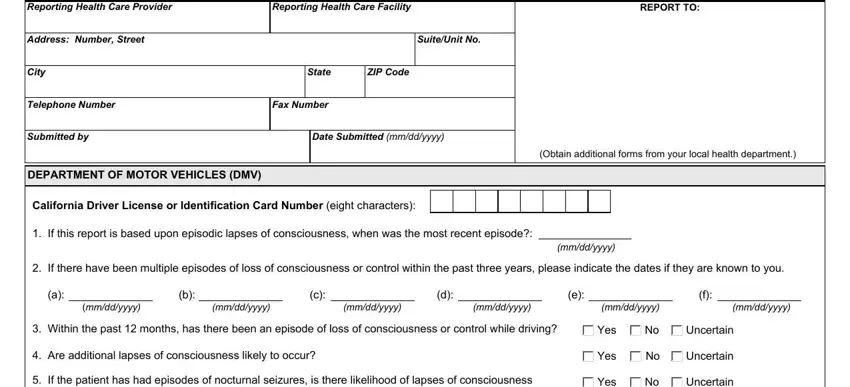
2. Once your current task is complete, take the next step – fill out all of these fields - Reporting Health Care Provider, Reporting Health Care Facility, REPORT TO, Address Number Street, SuiteUnit No, City, State, ZIP Code, Telephone Number, Fax Number, Submitted by, Date Submitted mmddyyyy, DEPARTMENT OF MOTOR VEHICLES DMV, California Driver License or, and Obtain additional forms from your with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The following part is mostly about If the patient has had episodes, Has this patient been diagnosed, Would you currently advise this, Does this patients condition, Would you recommend a driving, Yes, Yes, Yes, Yes, Uncertain, Uncertain, Uncertain, Uncertain, Remarks, and CDPH c for reporting conditions - complete every one of these blank fields.
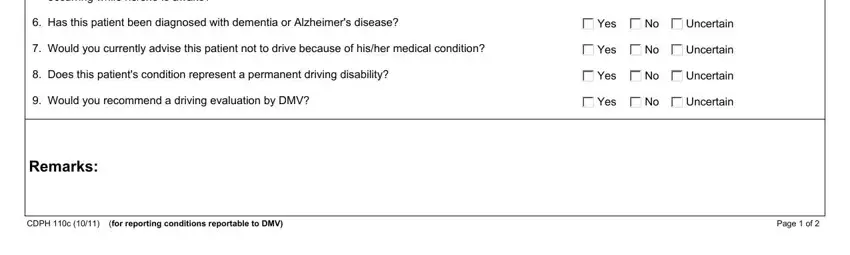
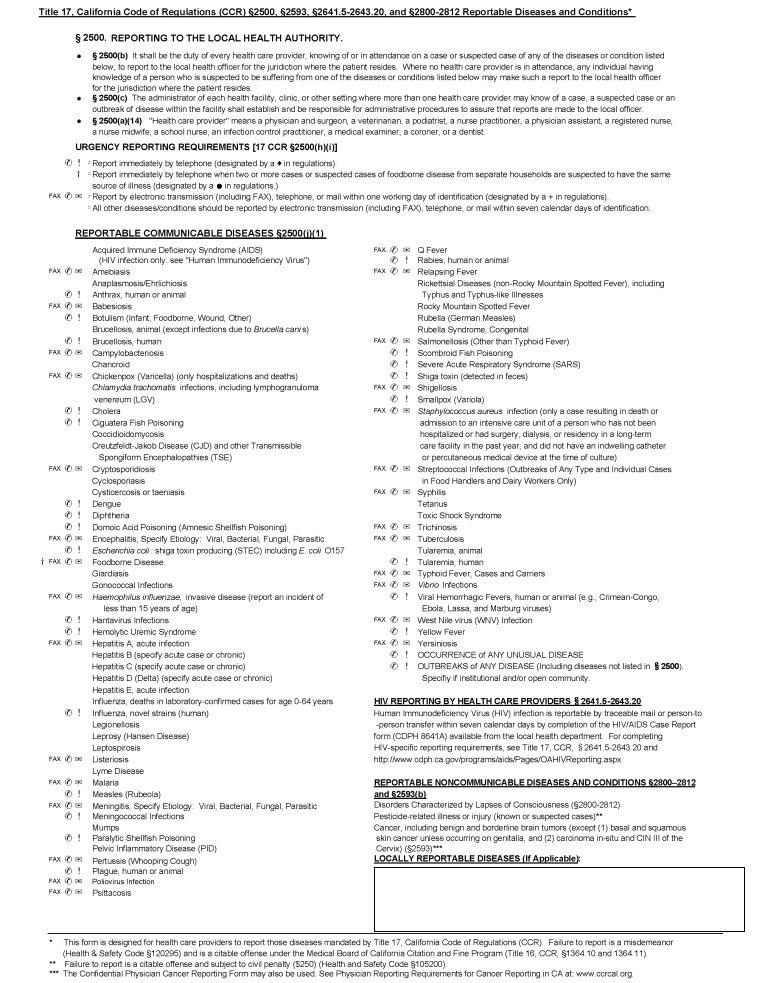
4. To move forward, this next stage requires filling in a few blanks. Included in these are CDPH c, and Page of, which you'll find essential to moving forward with this PDF.
People frequently get some points wrong while filling out CDPH c in this area. Be sure to revise what you type in right here.
Step 3: Confirm that the information is accurate and just click "Done" to proceed further. Right after registering afree trial account here, you will be able to download dmv morbidity report or send it through email at once. The form will also be at your disposal in your personal account page with your changes. FormsPal is devoted to the personal privacy of all our users; we make sure all personal data used in our editor continues to be protected.