a.Type or print all entries in BLOCK or CAPITAL LETTERS.
b.Accomplish this form in softcopy when making remittances to HDMF or to any authorized collecting agent based on the following payment schedule:
Schedule of Payments |
First Letter of |
Due Date |
Employer/Business Name |
10th to the 14th day of the month |
A to D |
E to L |
15th to the 19th day of the month |
M to Q |
20th to the 24th day of the month |
R to Z, Numeral |
25th to the end of the month |
c. For employer with branch offices, please prepare separate Membership Contributions Remittance Form (MCRF) for each branch indicating therein their respective addresses.
d. A separate MCRF should be accomplished per membership program, per period covered, per type of payment (whether cash or check payment) and in cases wherein Credit Memo shall be applied as payment to succeeding remittances to the Fund.
e. RATE OF MEMBERSHIP CONTRIBUTIONS (MC) |
|
MONTHLY COMPENSATION |
CONTRIBUTION RATE |
|
(BASIC + COLA) |
EMPLOYEE |
EMPLOYER |
TOTAL |
P1,500.00 and below |
1% |
2% |
3% |
Over P1,500.00 |
2% |
2% |
4% |
The maximum Monthly Compensation to be used in computing the employee and employer contributions shall not be more than 5,000.00.
A member may contribute more than what is required, however the employer shall only be mandated to contribute two percent (2%) of the monthly compensation of the member as counterpart contribution. In case the member increases his/her monthly membership contribution, the employer shall have the option to match said increase or to contribute only what is required.
f.Membership contribution payments to be remitted should be equal to the total amount reflected in the MCRF. Check payments should be made payable to HDMF and shall be posted upon clearing.
g. Employers with over remittance from previous payments shall be issued with a Notice of Overpayment and Credit Memo. For remittances previously made for employees for whom remittances should not have been made, the employer shall request a refund subject to the Fund’s verification and approval. The request shall be made not later than six (6) months from the time said remittance was made.
h. Employers who shall remit on or before the due date as evidenced by the validated Membership Contribution Remittance Form (MCRF) or Pag-IBIG Fund Receipt shall be entitled to an incentive fee equivalent to 0.2% of the amount remitted provided he satisfy all the conditions required.
|
|
|
|
|
|
1 |
|
|
2 |
|
|
|
|
3 |
|
|
4 |
|
|
|
|
5 |
|
|
6 |
|
|
|
|
7 |
|
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
i.Failure or refusal of the Employer to pay or to remit the contributions herein prescribed shall not prejudice the right of the covered employee to the benefits under the Fund. Such Employer shall be charged a penalty equivalent to 1/10 of 1% per day of delay of the amount due starting on the first day immediately following the due date until the date of full settlement.
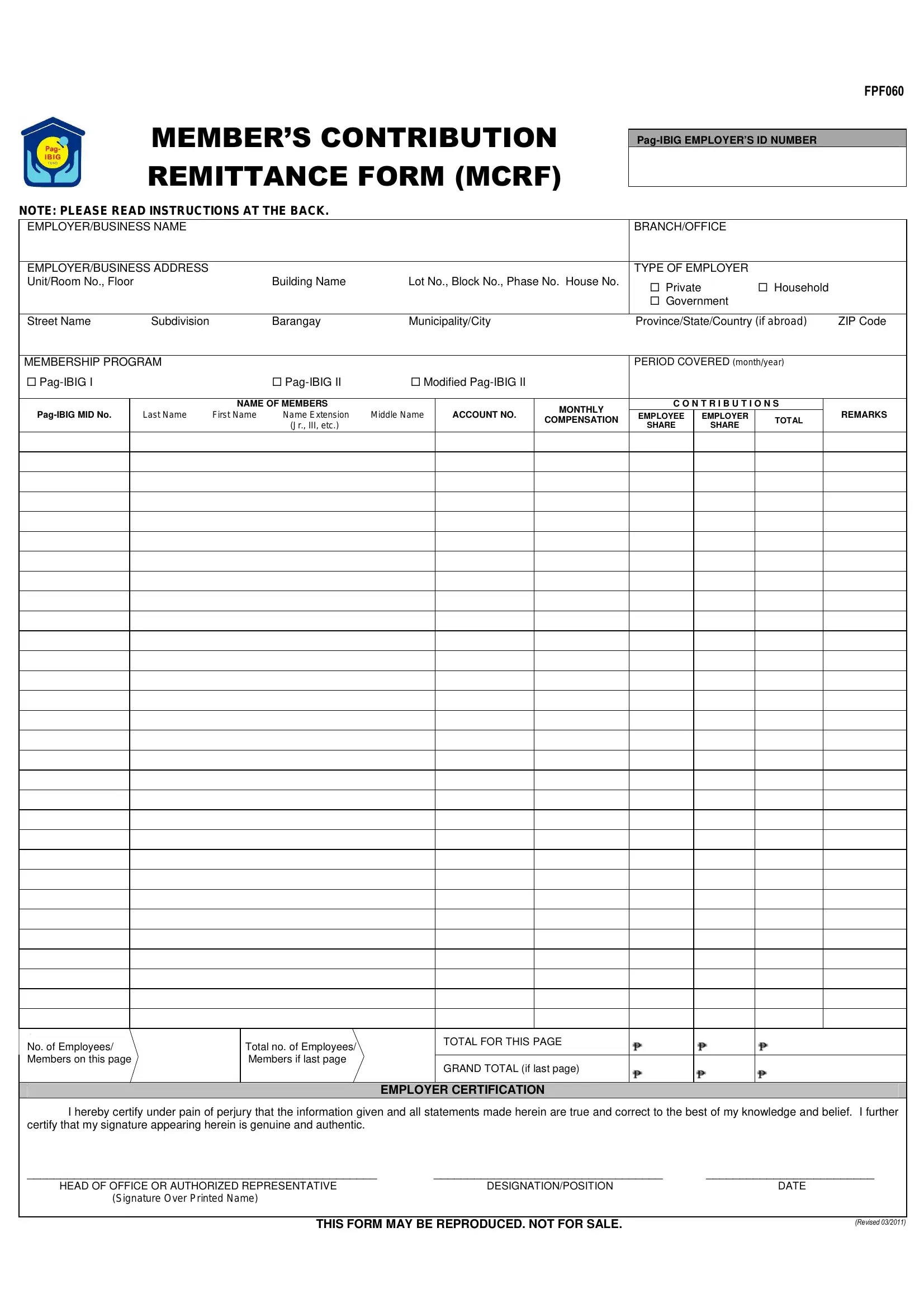
1Pag-IBIG Employer’s ID No. – assigned Pag-IBIG Employer’s ID Number.
2Employer/Business Name – per DTI/SEC Registration.
3Branch/Office Assignment – indicate what branch or office the remitting employer/business/company is assigned.
4Employer/Business Address - indicate Unit/Room No., Floor, Building Name or Lot No., Block No., Phase No. or House No. and Street Name, Subdivision, Barangay, Municipality/City, Province, and ZIP Code.
5Type of Employer – indicate whether Private, Government or Household employer.
6Membership Program – indicate if MC remittance is for Pag-IBIG I, Pag-IBIG II or Modified Pag-IBIG II program.
7Period Covered – indicate the applicable month and year of MC remittance.
8Pag-IBIG MID No. - indicate the member’s assigned Pag-IBIG Membership Identification (MID) Number.
9Name of Members - indicate member’s complete name in the following format: Last Name, First Name, Name Extension (Jr., III, etc.), Middle Name
10Account No. - accomplish this column only if the member has multiple Modified Pag-IBIG II (MP2) accounts. Indicate the Account No. for the applicable remittance period.
11Monthly Compensation – refer to the basic salary and other allowances, where basic salary includes, but is not limited to, fees, salaries, wages, and similar items received in a month. Accomplish this portion only when remitting the member’s initial membership contribution or if there are changes in monthly compensation of the member.
12-14 |
Contributions – indicate the amount of employee contributions |
|
under column |
12 |
, the amount of employer contributions under |
|
column 13 , |
and |
the |
total amount of employee and employer |
|
contributions under |
14 |
. Do not round-off nor drop centavos. |
15Remarks - accomplish this portion only to report changes in the employee’s/member’s employment status and to update any information regarding the employee/member. Indicate the appropriate code and effectivity date in the following format (mm/dd/yy) on the space provided for. Please refer to the following codes and examples:
N |
- Newly Hired |
Examples |
L |
- Leave Without Pay/AWOL |
1. |
N: |
1/4/2010 |
RS |
- Resigned/Separated |
2. L: |
1/21/2010 |
RT |
- Retired |
3. |
RS: 1/3/2010 |
D |
- Deceased |
4. |
D: |
1/14/2010 |
O- Others, please specify reason
16Indicate the number of members listed in this page.
Indicate the total number of members listed if this is the last page of
17the listing.
18Indicate the total amount due and employer contributions per page
19Indicate the grand total amount due and employer contributions if this is the last page
20Employer Certification - to be accomplished and duly signed by the Head of Office/Authorized Representative.