
You can complete the pag ibig payment form quickly using our online PDF tool. Our team is committed to providing you with the best possible experience by continuously improving the editor. Here is how to get started.
What You Need Before Starting
Gather these details before opening the form:
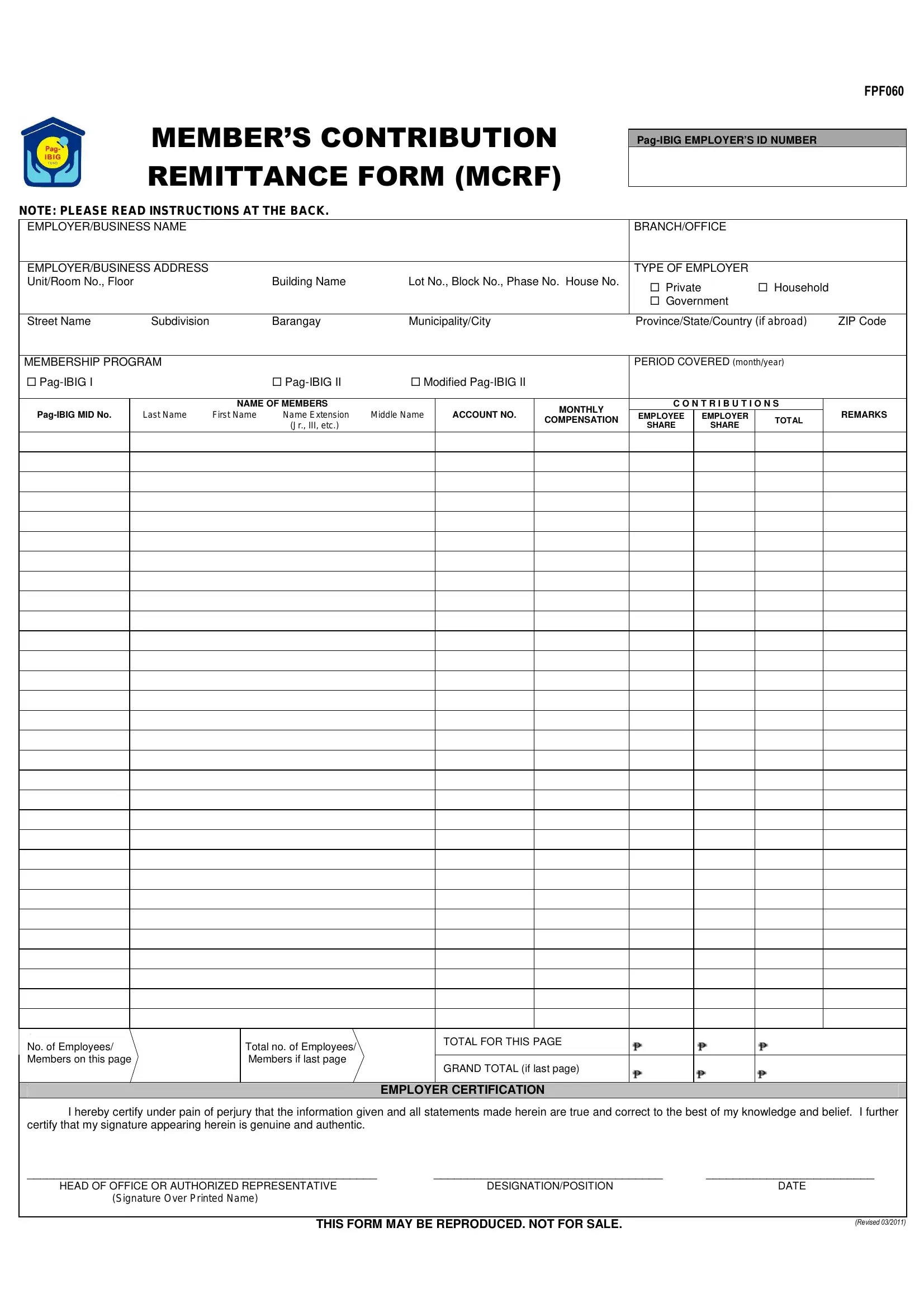
- Your Pag-IBIG Employer ID Number
- Names and monthly salaries of all covered employees
- The contribution period (month and year)
- Employee share (1%) and employer share (2%) per member
How to Complete the Form Step by Step
Step 1: Click "Get Form" at the top of the page. The form opens in the online PDF editor.
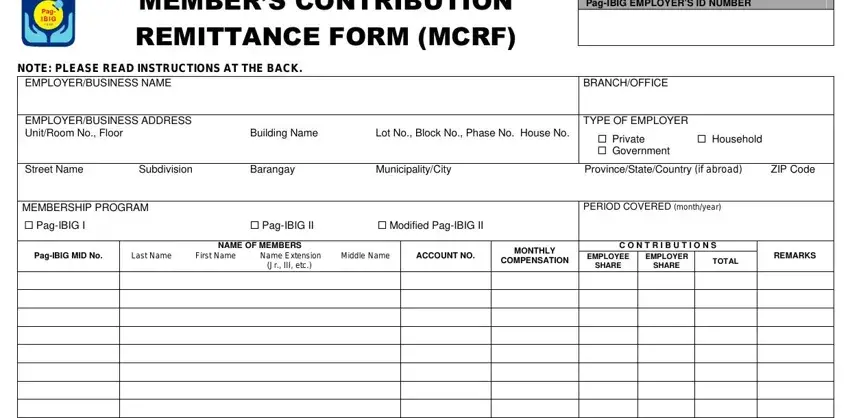
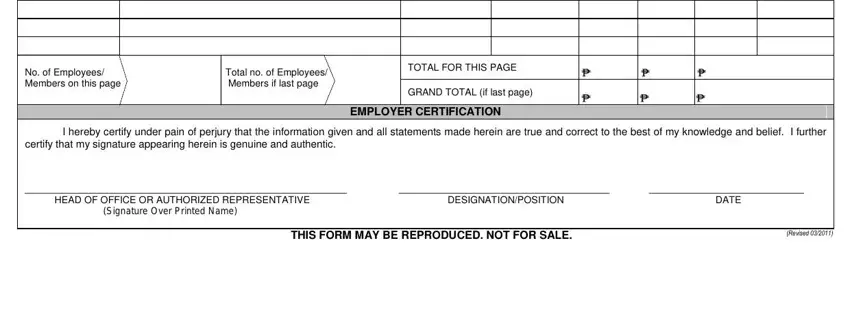
Step 2: Enter your employer information in the top section. Add each employee's name, monthly compensation, and contribution amounts in the rows below. Double-check the No. of Employees/Members count on each page before moving on.
Step 3: Complete the last section. Fill in the Grand Total and the Employer Certification fields. Click "Done" when you are finished. You can then download, print, or email the completed form.
Related Philippine Employer Forms
Philippine employers must file contributions to several agencies each month. These related forms are also available on FormsPal:
- SSS Contribution Form R-3 for Social Security System remittances
- CF1 PhilHealth Form for employee health insurance contributions
- Pag-IBIG Members Data Form for enrolling new employees in the Pag-IBIG Fund
- Pag-IBIG MP2 Renewal Form for Modified Pag-IBIG II program participants
- HQP-PFF-162 Form for Pag-IBIG housing loan applications
Submit the completed form to any Pag-IBIG Fund branch or via the Virtual Pag-IBIG portal. FormsPal keeps your information private and does not share it with third parties.