


 Insurance
Insurance  Employment, School, or Military
Employment, School, or Military 
 Member/Applicant/Volunteer
Member/Applicant/Volunteer  Personal Use, Court, or Attorney
Personal Use, Court, or Attorney 
 TNC
TNC


 POLICE CRASH REPORT
POLICE CRASH REPORT
 I was a DRIVER.
I was a DRIVER.
 I legally REPRESENT a person injured or involved in the crash.
I legally REPRESENT a person injured or involved in the crash.
 I am the parent or legal guardian of a
I am the parent or legal guardian of a 
 I was a PASSENGER.
I was a PASSENGER. I was injured in the crash or as a result thereof (ex: injured pedestrian).
I was injured in the crash or as a result thereof (ex: injured pedestrian). 
 I am the owner of a vehicle/property involved in the crash.
I am the owner of a vehicle/property involved in the crash.
 I am the personal representative (guardian, executor, next of kin, etc.) of a person injured or killed in the crash.
I am the personal representative (guardian, executor, next of kin, etc.) of a person injured or killed in the crash.
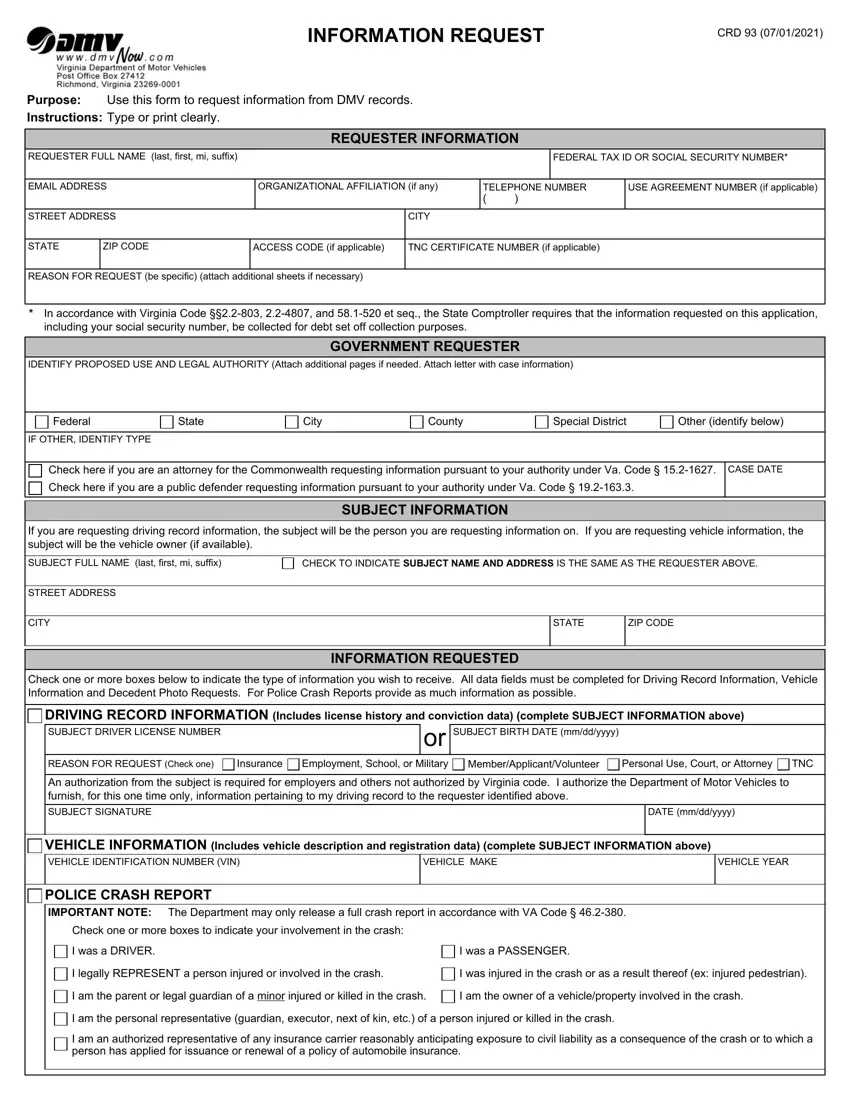
It is easy to fill out documents taking advantage of our PDF editor. Updating the crd93 form is simple in the event you try out the following actions:
Step 1: Click the button "Get Form Here".
Step 2: So you are on the form editing page. You may modify and add information to the form, highlight words and phrases, cross or check specific words, add images, put a signature on it, delete unrequired fields, or eliminate them completely.
The following segments will compose the PDF form that you'll be creating:
The system will need you to prepare the Federal, State, City, County, Special District, Other identify below, IF OTHER IDENTIFY TYPE, Check here if you are an attorney, CASE DATE, Check here if you are a public, If you are requesting driving, SUBJECT FULL NAME last first mi, CHECK TO INDICATE SUBJECT NAME AND, SUBJECT INFORMATION, and STREET ADDRESS section.
You will have to write particular particulars in the field An authorization from the subject, DATE mmddyyyy, VEHICLE INFORMATION Includes, VEHICLE MAKE, VEHICLE YEAR, POLICE CRASH REPORT IMPORTANT NOTE, Check one or more boxes to, I was a DRIVER, I was a PASSENGER, I legally REPRESENT a person, I was injured in the crash or as a, I am the parent or legal guardian, I am the owner of a, I am the personal representative, and I am an authorized representative.
The CRD, CRASH DATE mmddyyyy TIME OF CRASH, INFORMATION REQUESTED continued, CITYCOUNTYTOWN WHERE CRASH, DRIVER LICENSE NUMBER, PASSENGERPEDESTRIAN FULL NAME last, PASSENGERPEDESTRIAN FULL NAME last, PASSENGERPEDESTRIAN FULL NAME last, PASSENGERPEDESTRIAN FULL NAME last, DECEDENT PHOTO REQUEST requester, DECEDENT FULL NAME last first mi, DECEDENT DMV CUSTOMER NUMBER, DECEDENT BIRTH DATE mmddyyyy, Requesters relationship to, and Executor Administrator area is the place where all sides can place their rights and responsibilities.
Check the sections CERTIFICATION I understand that it, REQUESTER SIGNATURE, DATE mmddyyyy, CUSTOMER RECORDS FEES, Driving Record Vehicle Record, Supporting Documents per page, PAYMENT METHODS If you are mailing, CHECK Made payable to DMV, ENTER CHECK AMOUNT, MONEY ORDER Made payable to DMV, ENTER MONEY ORDER AMOUNT, Proof of Requesters Identification, DMV CUSTOMER SERVICE CENTER USE, Valid Drivers License Number, and Other Photo Identification and then fill them out.
Step 3: Choose the "Done" button. Finally, you may transfer the PDF file - upload it to your device or deliver it via email.
Step 4: Get copies of the template. This would prevent forthcoming troubles. We do not see or share your data, for that reason be assured it's going to be protected.
