
Completing this California child aid application online is straightforward using our PDF tool. Anyone can fill out the form here in just a few minutes. Our tool is continuously updated to provide the best user experience, incorporating feedback from thousands of California families who use it to access Cash Aid and CalFresh benefits for their children.
Steps to Fill Out the Application
Step 1: Access the application in our editor by clicking the "Get Form" button at the top of this page.
Step 2: Use our PDF editor to fill in all required fields. You can add custom text, adjust existing entries, insert information about the child, and sign the document digitally.
This application requires you to enter specific information. To ensure accuracy and completeness, keep the following in mind:
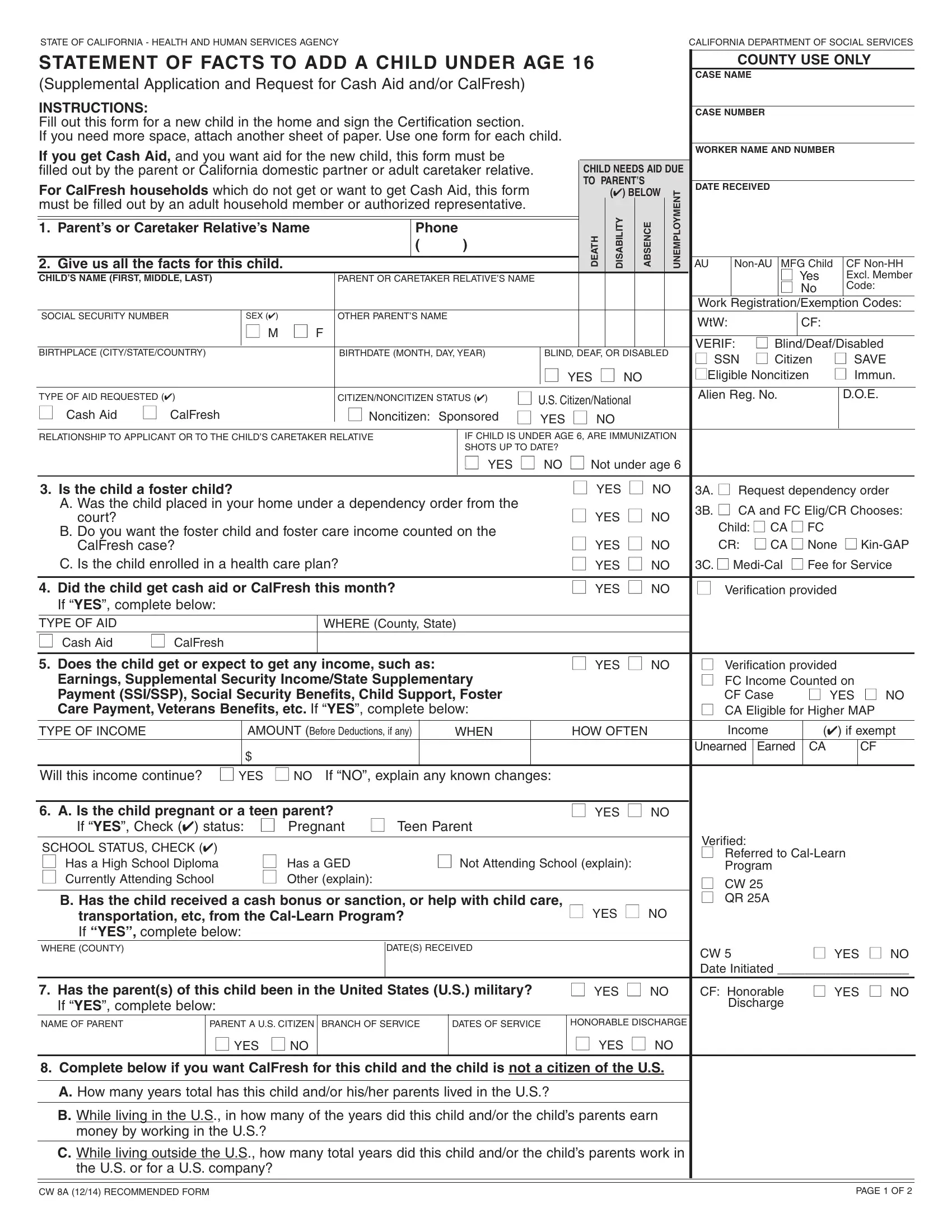
1. Begin completing the application with the essential fields. Gather all information you need and confirm that nothing is missing.
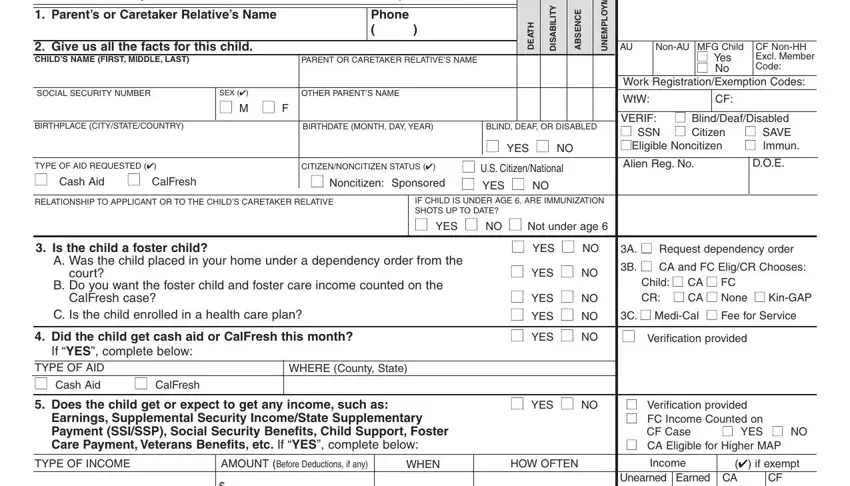
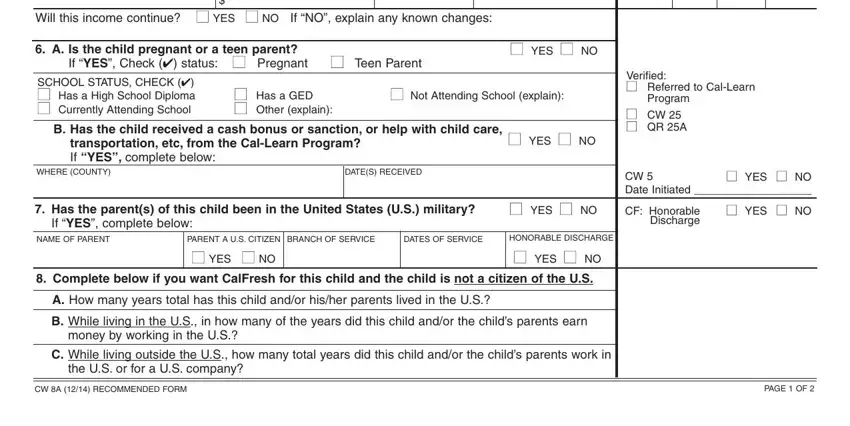
2. The next section includes fields for: income continuation status, pregnancy or teen parent status, school attendance details, prior cash aid or transportation received, parental information, and county details. Fill in each field with accurate information.
3. In this section, provide details about the child's resources: property, land, bank accounts, trust funds, Medicare or health insurance coverage, and county-use fields. Fill in these sections with the greatest attention to detail.
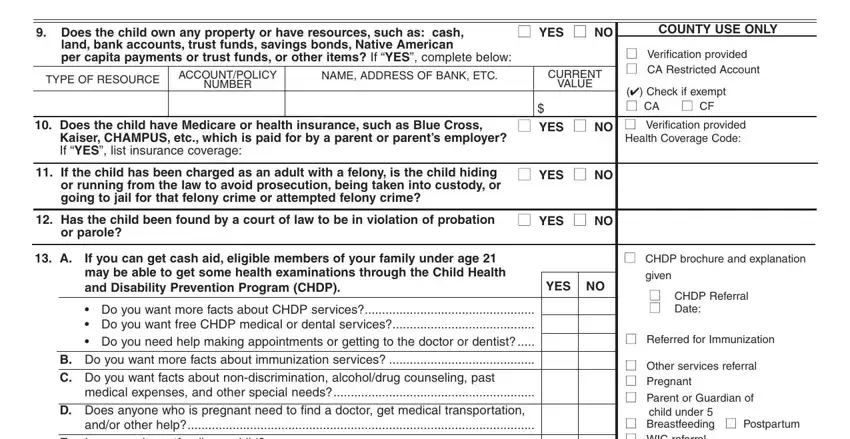
4. Begin the fourth section by completing all remaining fields for family planning services, WIC breastfeeding programs, and the certification statement. The certification must be signed by the caretaker or relative under penalty of perjury.
5. In the final section, complete the remaining signature fields for the cash-aided spouse or partner, a witness to mark, and the county worker. The county use section covers eligibility determination, effective date of aid, and authorization date.
Step 3: Once all blanks are filled, click "Done" to finalize the application. Create a free account to save your completed application and access it anytime from your personal account. All information is stored securely on our platform.
Frequently Asked Questions
What benefits does this form cover?
This application covers Cash Aid (CalWORKs) and CalFresh food assistance for eligible children under age 16 living in California households already receiving aid.
How many fields does the application have?
The form contains 192 fillable fields and takes approximately 39 minutes on average to complete. Fill out the application carefully to avoid delays in processing.
What related California welfare forms might I need?
Related forms include the CW 42 form for reporting aid changes and the DCFS CW form CPI-2 for child protective services cases. You may also need the CalFresh application if you are applying for food assistance as a new applicant rather than adding to an existing case.