Cy 131 Form is an important document for any taxpayer, whether it be an individual or a business. This form is used to calculate the amount of tax that is owed to the government. The Cy 131 Form must be filed by April 15th each year. Failing to file this form on time can result in steep penalties and fines. Make sure you are aware of your obligations and Deadline! Thank you for reading! If you have any further questions, please feel free to contact our office. We would be happy to help!
| Question | Answer |
|---|---|
| Form Name | Cy 131 Form |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | cy131update, PENNSYLVANIA, CW, Islander |
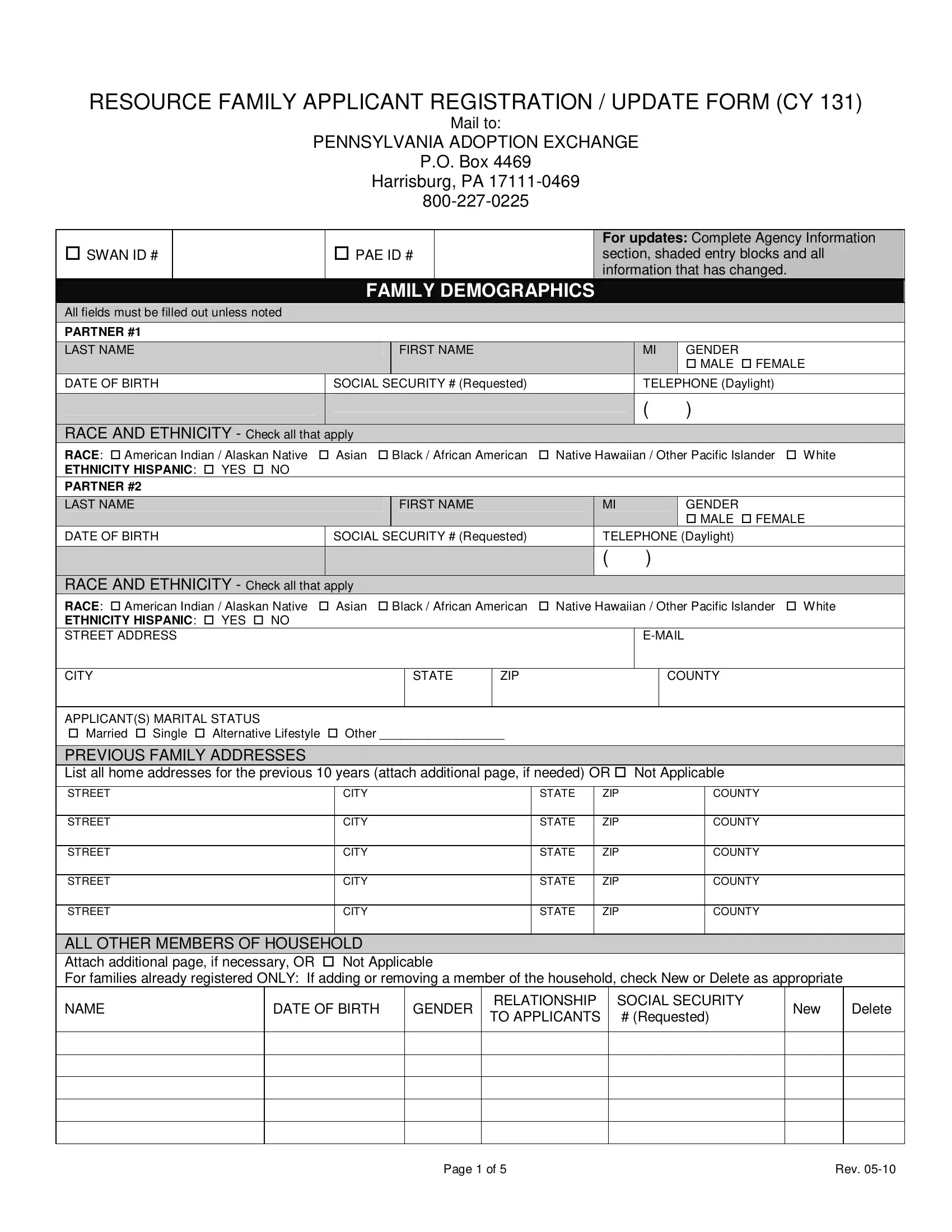
RESOURCE FAMILY APPLICANT REGISTRATION / UPDATE FORM (CY 131)
Mail to:
PENNSYLVANIA ADOPTION EXCHANGE
P.O. Box 4469
Harrisburg, PA
SWAN ID #
PAE ID #
For updates: Complete Agency Information
section, shaded entry blocks and all information that has changed.
FAMILY DEMOGRAPHICS
All fields must be filled out unless noted
PARTNER #1
LAST NAME
DATE OF BIRTH
FIRST NAME
SOCIAL SECURITY # (Requested)
MI |
GENDER |
MALE FEMALE
TELEPHONE (Daylight)
( )
RACE AND ETHNICITY - Check all that apply
RACE: American Indian / Alaskan Native |
Asian |
Black / African American |
Native Hawaiian / Other Pacific Islander |
White |
|||||
ETHNICITY HISPANIC: YES NO |
|
|
|
|
|
|
|
|
|
PARTNER #2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
FIRST NAME |
|
MI |
|
GENDER |
|
|
|
|
|
|
|
|
|
MALE FEMALE |
|
DATE OF BIRTH |
|
SOCIAL SECURITY # (Requested) |
|
TELEPHONE (Daylight) |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
RACE AND ETHNICITY - Check all that apply |
|
|
|
|
|
|
|
||
RACE: American Indian / Alaskan Native |
Asian |
Black / African American |
Native Hawaiian / Other Pacific Islander |
White |
|||||
ETHNICITY HISPANIC: YES NO |
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
CITY
STATE
ZIP
COUNTY
APPLICANT(S) MARITAL STATUS
Married Single Alternative Lifestyle Other __________________
PREVIOUS FAMILY ADDRESSES
List all home addresses for the previous 10 years (attach additional page, if needed) OR Not Applicable
STREET
CITY
STATE
ZIP
COUNTY
STREET
CITY
STATE
ZIP
COUNTY
STREET
CITY
STATE
ZIP
COUNTY
STREET
CITY
STATE
ZIP
COUNTY
STREET
CITY
STATE
ZIP
COUNTY
ALL OTHER MEMBERS OF HOUSEHOLD
Attach additional page, if necessary, OR Not Applicable
For families already registered ONLY: If adding or removing a member of the household, check New or Delete as appropriate
NAME |
DATE OF BIRTH |
GENDER |
RELATIONSHIP |
SOCIAL SECURITY |
New |
|
TO APPLICANTS |
# (Requested) |
|||||
|
|
|
|
|||
|
|
|
|
|
|
Delete
Page 1 of 5 |
Rev. |
FAMILY INFORMATION
Please answer the following questions.
1.List the occupations of the applicants, including a
Partner 1 __________________________________
Partner 2 __________________________________
2.List any special needs training applicants have.
3. Select the type of neighborhood where applicants live. |
Rural |
|||
FAMILY DISPOSITION |
|
|
|
|
Disposition: |
APPROVED |
DISAPPROVED |
CLOSED |
|
For type of care: |
ADOPTIVE |
FOSTER CARE |
KINSHIP |
|
Urban Suburban
DATE of DISPOSITION
Please choose type of foster care approval or reason for any disapproval or closure below.
APPROVED - For foster care, choose type of approval
FULL
REGULATION WAIVER GRANTED
DISAPPROVED - Choose reason
CHILD ABUSE HISTORY
CRIMINAL HISTORY
FAILURE TO COMPLETE TRAINING
FAILURE TO FOLLOW AGENCY POLICY
FALSIFICATION / MISREPRESENTATION OF INFORMATION
UNFAVORABLE FAMILY PROFILE
OTHER Explain:
________________________
CLOSED - Choose reason
Adopted child from PA child welfare system
Adopted child from another state (CW)
Adopted privately / domestically
Adopted internationally
Kinship adoption
Kinship care – not adoption
Kinship
Permanent Legal Custodian
Family unresponsive
Moved to other agency
Moved away
No longer interested / personal reasons
Other reason: __________________
If closing a previously registered, approved family, complete all shaded areas of the form and the Agency Information section. Sign and date below. I certify that the information provided is accurate and complete.
Signature______________________________________ Date _________________________
FOSTER FAMILY APPEAL ACTIVITY
FAMILY FILED APPEAL
LIST ANY RESTRICTIONS TO APPROVAL
BASIS FOR APPEAL
REGISTERING AGENCY
APPEAL UPHELD |
DATE |
APPEAL DENIED |
|
AGENCY INFORMATION
REGISTERING AGENCY |
|
|
|
|
CASEWORKER (Full name) |
|
|
|
|
|
|
MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP |
|
COUNTY |
|
|
|
|
|
|
TELEPHONE # |
|
|
|
FAX # |
|
( |
) |
|
|
|
|
ALL PREVIOUS FOSTER CARE / ADOPTION AGENCY AFFILIATIONS or Not Applicable Attach additional page, if needed
PREVIOUS AGENCY |
|
|
|
|
CASEWORKER (Full name) |
|
|
|
|
|
|
MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP |
|
COUNTY |
|
|
|
|
|
|
TELEPHONE # |
|
|
|
FAX # |
|
( |
) |
|
|
|
|
Page 2 of 5 |
Rev. |
ALL PREVIOUS FOSTER CARE / ADOPTION AGENCY AFFILIATIONS (continued)
PREVIOUS AGENCY
MAILING ADDRESS
CITY
TELEPHONE #
( )
STATE
ZIP
FAX #
CASEWORKER (Full name)
COUNTY
TYPE OF CHILD APPROVED FOR FAMILY
WHAT IS THE MAXIMUM NUMBER OF CHILDREN APPROVED FOR THIS FAMILY’S HOME? ___________
SPECIAL NEEDS
CHECK ALL SPECIAL NEEDS FAMILY IS APPROVED TO PROVIDE. |
NOT APPLICABLE |
||
ABUSE HISTORY |
NEGLECT HISTORY |
|
|
ALCOHOL EXPOSED |
PHYSICAL DISABILITY |
|
|
DRUG EXPOSED INFANT |
RUNAWAY HISTORY |
|
|
EMOTIONAL DISABILITY |
SEXUAL ABUSE HISTORY |
|
|
HIV |
SIBLINGS: # _____________ |
|
|
MH DIAGNOSIS |
SPECIAL EDUCATION STUDENT |
|
|
MR DIAGNOSIS |
SPECIAL MEDICAL CARE |
|
|
MULTIPLE PLACEMENT HISTORY
OTHER: __________________________________________________
TYPE OF CHILD FAMILY PREFERS - If family is disapproved, check Not Applicable
RACE / ETHNICITY - Check all family will accept
RACE:
AMERICAN INDIAN / ALASKAN NATIVE
ASIAN
BLACK / AFRICAN AMERICAN
NATIVE HAWAIIAN / OTHER PACIFIC ISLANDER
WHITE
ETHNICITY HISPANIC: YES NO
GENDER
MALE
FEMALE
EITHER
NUMBER OF CHILDREN & AGE RANGE
AGE RANGE:
BETWEEN ______ and _____ YEARS
NUMBER OF CHILDREN:
SINGLE CHILD
SIBLINGS
MAXIMUM NUMBER _________
STOP HERE if match suggestions are not needed
CHARACTERISTICS OF CHILD
For adoptive families only: Please choose from the characteristics listed to tell us the type of child the family wants to adopt. Place an X in the most appropriate box for each characteristic.
HEALTH
Characteristic
1.No significant health problems
2.Allergies or asthma (may require treatment)
3.Hyperactivity (may require treatment)
4.Speech problems (may require treatment)
5.Hearing problems (may require treatment)
6.Legally deaf
7.Vision problems (may require treatment)
8.Legally blind
9.Dental problems (may require treatment)
10.Orthopedic problems (special shoes, brace, etc.)
11.Seizure disorder
Acceptable
Will
Consider
Unacceptable
Page 3 of 5 |
Rev. |
|
EDUCATION |
|
|
Characteristic |
Acceptable |
Will |
|
Consider |
|||
|
|
12.High achiever
13.Achieves on grade level in regular classes
14.Achieves below grade level in regular classes
15.Needs special education classes
16.Needs learning disability classes (LD)
17.Needs classes for the emotionally or behaviorally handicapped
18.Needs tutoring in one or more subjects
19.Has serious behavior problems at school
Unacceptable
CHARACTERISTICS AND BEHAVIORS
Characteristic |
Acceptable |
Will |
Unacceptable |
|
Consider |
||||
|
|
|
20.Generally quiet and shy
21.Generally outgoing and noisy
22.Emotional issues require ongoing therapy
23.Tends to reject father figures
24.Tends to reject mother figures
25.Difficulty making friends and relating to other children.
26.Frequently wets the bed.
27.Frequently wets during the day
28.Frequently soils him/herself
29.Masturbates frequently or openly
30.Poor social skills
31.Problem with lying
32.Problem with stealing
33.Frequently starts physical fights with other children
34.Tends to abuse animals
35.Tends to be destructive of clothing, toys. etc.
36.Frequently uses foul or bad language
37.Frequent temper tantrums
38.Difficulty accepting and obeying rules
39.History of inappropriate sexual behavior
40.History of running away
41.History of playing with matches, setting fires
FAMILY CONNECTEDNESS & HISTORY
Characteristic |
Acceptable |
42.Strong ties to birth family
43.Strong ties to foster family
44.Needs continued contact with siblings
45.Previous adoptive disruption
46.Sexually abused
47.Exposed to promiscuous sexual behavior
48.Conceived by rape
49.Conceived as a result of prostitution
Will
Consider
Unacceptable
Page 4 of 5 |
Rev. |
50. One or both parents addicted to alcohol
FAMILY CONNECTEDNESS & HISTORY
Characteristic
51.One or both parents chemically dependent, other than alcohol
52.One or both parents has criminal record
53.One or both parents mentally retarded
54.One or both parents has mental illness
55.No information available about one or more parent
Acceptable
Will
Consider
Unacceptable
RESOURCE FAMILY’S FEELINGS ABOUT OPENNESS WITH BIRTH FAMILY
Characteristic
56.Meet with birth parents
57.Contact with birth parents through agency or intermediary
58.Send letters to birth parents
59.Receive letters from birth parents
60.Send videos to birth parents
61.Receive videos from birth parents
62.Have phone contact between adults
63.Child continues visits with siblings
64.Child continues visits with extended relatives in birth family
65.Child continues visits with birth parents
66.Receive birth parents’ name, address, phone number, etc.
67.Adoptive parents willing to give first name to birth parents
68.Adoptive parents willing to give identifying information to birth parents
Acceptable
Will
Consider
Unacceptable
SIGNATURE OF AGENCY WORKER REQUIRED
I verify that this information is accurate and complete to the best of my knowledge or information and belief. The information is submitted as true and correct under penalty of law (Section 4904 of the Pennsylvania Crimes Code).
_______________________________________ |
________________ |
AGENCY WORKER |
DATE |
|
|
Page 5 of 5 |
Rev. |