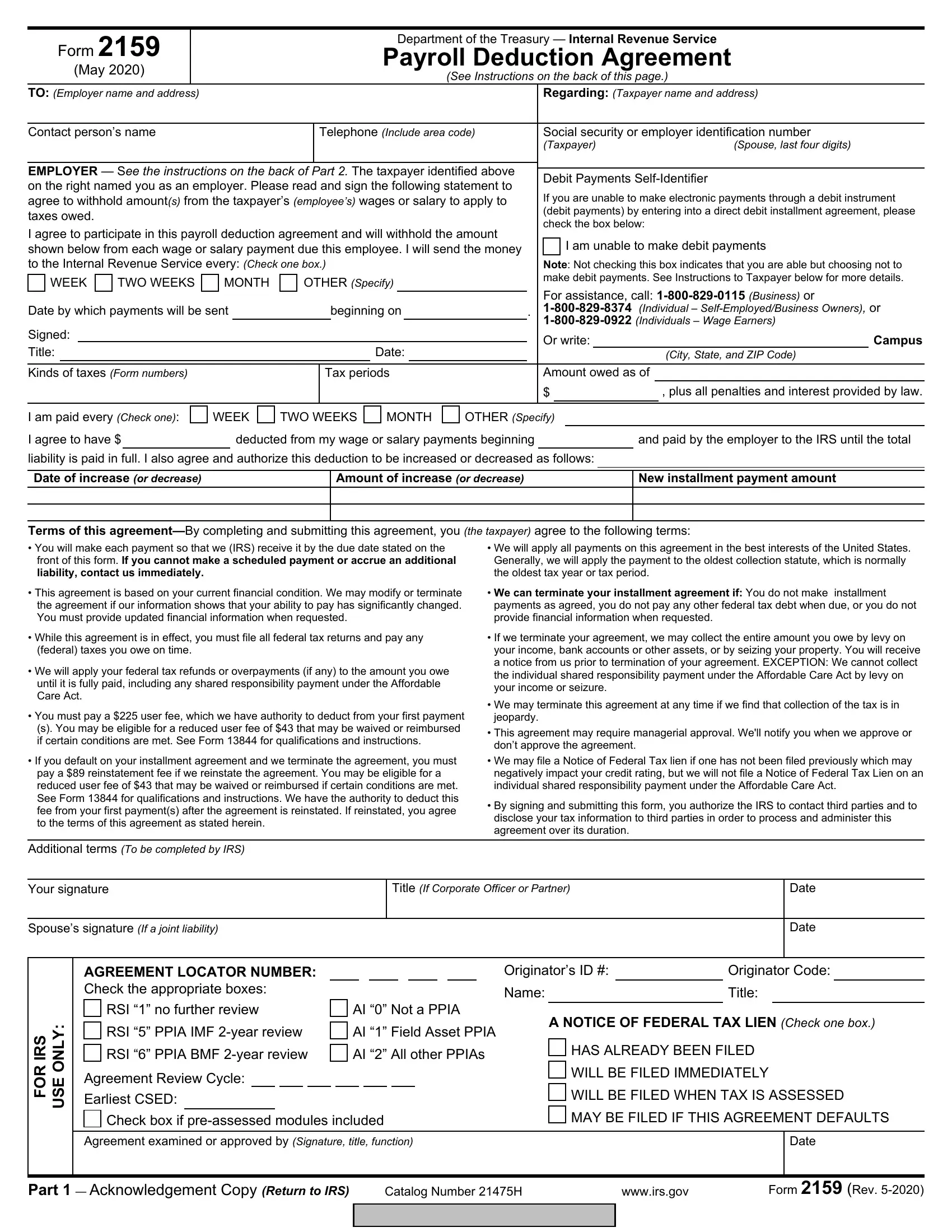
The IRS Form 2159, known as the Payroll Deduction Agreement, is a crucial tool for taxpayers who owe taxes and are seeking a manageable way to fulfill their obligations through deductions from their wages or salary. Updated in May 2020, this form facilitates an arrangement between taxpayers and the Internal Revenue Service, allowing for the direct withholding of tax payments by an employer from an employee's paycheck. Crucial to initiating this agreement is the requirement for both employer and employee consent, as outlined in detailed instructions provided on the form itself. The form also sets out various terms of agreement, including the payment schedule, amounts to be deducted, and the specific types of taxes and periods covered. Employers are tasked with forwarding withheld amounts to the IRS at agreed intervals, which could be weekly, bi-weekly, monthly, or as otherwise specified. Importantly, the form contains sections that address potential adjustments to the deduction amounts, criteria under which the agreement might be terminated or modified by the IRS, and information concerning fees associated with the agreement, such as the user fee and possible reinstatement fee. Notably, the agreement allows the IRS to apply federal tax refunds or overpayments towards the tax liability and describes conditions under which a Notice of Federal Tax Lien might be filed, which could impact the taxpayer's credit rating. In essence, Form 2159 is designed to offer a structured and systematic approach to paying down tax debt, ensuring compliance while mitigating the financial burden on taxpayers.
| Question | Answer |
|---|---|
| Form Name | Irs Form 2159 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | irs form 2159, 2159, form ftc gov complaint, id theft complaint |