In order to protect the safety of children and vulnerable adults, the state of New Mexico requires all individuals who work with these populations to have a background check. This includes individuals who work in daycare centers, schools, healthcare facilities, and other organizations that interact with minors or vulnerable adults. The process of getting a background check is simple, and can be completed online in just a few minutes. In this blog post, we will walk you through the steps of completing a Cyfd Background Check Form. Let's get started!
| Question | Answer |
|---|---|
| Form Name | Cyfd Background Check Form |
| Form Length | 20 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 5 min |
| Other names | ececd background check unit, cyfd background check unit new mexico, cyfd background, nm cyfd background check |

Licensed
Background Check
and
Fingerprint Instructions
IF YOU HAVE QUESTIONS ABOUT YOUR BACKGROUND CHECK, CONTACT:
Background Check Unit
Phone: (505)
Fax: (505)
Address: P.O. Drawer 5160
Santa Fe, NM
Si usted necesita ayuda a completar este paquete, por favor llame (505)
CYFD Background Check Unit |
07/30/2010 |
LICENSED CHILDCARE HOMES AND FACILITIES
State and Federal laws prohibit the disclosure of information reviewed as a result of a background check and require security of records containing this information.
Completed fingerprint cards and accompanying information are legal documents. All documents submitted to the Children, Youth and Families Department become the property of the Department. The fingerprint cards and forms cannot be altered by anyone other than the applicant, and must clearly state the reason fingerprinted as “Employment in a Licensed Facility” or “Employment in a Licensed Childcare Home.”
The licensed center or home will receive a letter from the background check unit that indicates whether the applicant is eligible to provide childcare.
Privacy Act Statement
Children, Youth and Families Department’s (CYFD) request for your social security number (SSN) is made under the New Mexico Children’s and Juvenile Facility Criminal Records Screening Act, Section
CYFD Background Check Unit |
07/30/2010 |
PLEASE SUBMIT ALL REQUIRED FORMS AND FEES TO:
CHILDREN, YOUTH AND FAMILIES DEPARTMENT
ATTN: AS / BACKGROUND CHECK UNIT
P.O. DRAWER 5160
SANTA FE, NM
CHECKLIST
Have you included all of the following?
2 Fingerprint Cards
Applicant Written Statement
Employer Statement (to be filled out by employer if applying to work in a facility)
Dispositions (if applicable)
Money Order or Cashier’s Check
O$33.00 payable to CYFD
We will only accept one money order per applicant. Please do not combine money orders. Any money order received in the amount over $33.00 will be accepted; however, the excess amount is non- refundable.
Incomplete or illegible applications, or applications that are missing any of the required information or fees will be returned without further processing.
CYFD Background Check Unit |
07/30/2010 |
This is your physical address. Please include your mailing address in your application.
Employment in a Licensed Facility OR
Employment in a Licensed Childcare Home
NM920120Z
Child Care Lic Bu
Santa Fe, NM
CYFD Background Check Unit |
07/30/2010 |
FINGERPRINT CARD INSTRUCTIONS
1.Get Fingerprinted. Prints may be taken by some law enforcement agencies, including your local police department, sheriff’s office, or state police office. We encourage you to contact your local law enforcement agency to make arrangements for obtaining fingerprints. Use only the fingerprint cards included in this packet. Have at least one form of picture ID with you when you get fingerprinted. PLEASE NOTE: There may be a fingerprinting fee.
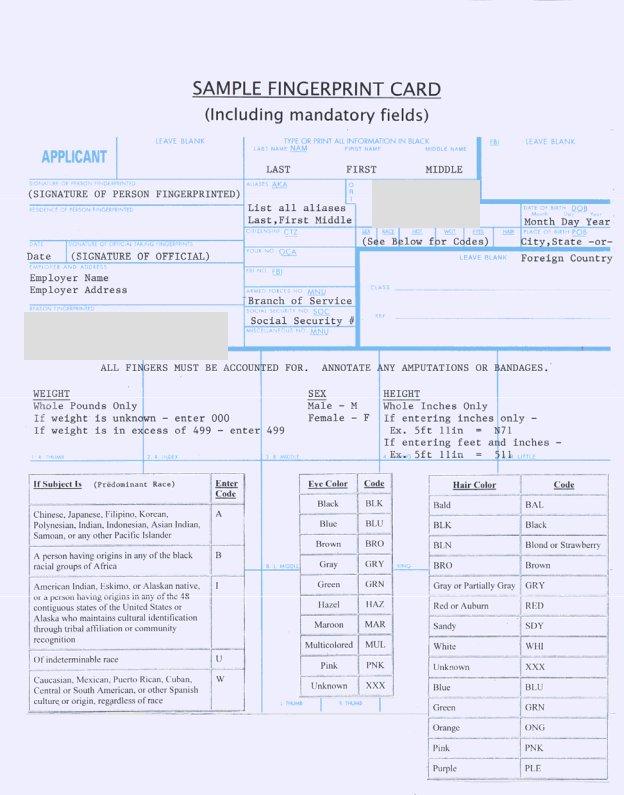
2.Complete the Top Portion of the Fingerprint Card IN BLACK INK. A sample fingerprint card is attached.
3.The fingerprint card must be typewritten or legibly printed. Illegible fingerprint cards will be rejected.
4.You must have two fingerprint cards.
REQUIRED INFORMATION:
LAST NAME: Complete last name. No abbreviations.
FIRST NAME: Complete first name. No abbreviations or nicknames.
MIDDLE NAME: Complete middle name. No initials, abbreviations, or nicknames. If you do not have a middle name, put “NMN.”
SIGNATURE OF PERSON FINGERPRINTED: Sign in the presence of the person who rolls your fingerprints.
RESIDENCE OF PERSON FINGERPRINTED: This is the physical address of the applicant. Please make sure to include your mailing address in another document, if different than the physical address. ALIASES USED BY THE APPLICANT: Include maiden name(s), nickname(s), previous married names, or any other name you have used.
CITIZENSHIP OF APPLICANT: Please identify your
citizenship by country. For example: United States, Mexico, Germany, Argentina, etc.
DATE OF FINGERPRINTING: The date the fingerprints are taken.
SIGNATURE OF OFFICIAL TAKING FINGERPRINTS: The person who rolls the fingerprints will sign this. EMPLOYER AND ADDRESS: This is the name and address of the employer, and this is the address the clearance/denial letters will be mailed to. Make sure it is the correct mailing address.
SOCIAL SECURITY NO: This is the social security number of the applicant.
SEX: Male or Female
RACE: Enter the race. See the sample fingerprint card for codes.
HEIGHT: Use whole inches only.
WEIGHT: Use whole pounds only.
EYE: See sample fingerprint card for codes.
HAIR: See sample fingerprint card for codes.
DATE OF BIRTH: Enter the date of birth of the applicant. Include month, day and year.
PLACE OF BIRTH: Enter the city and state, or, if outside the United States, enter the country.
REASON FINGERPRINTED:
Enter “Employment in a Licensed Facility” or “Employment in a Licensed Childcare Home.”
ENTER THE FOLLOWING INFORMATION ONLY IF IT APPLIES TO YOU:
ARMED FORCES NO: If you have an armed forces number, enter it here. Otherwise, if you served in the military, enter the branch here.
FBI NO: Enter your FBI number, if you have one.
MISCELLANEOUS NO: If you have another identifying number (i.e. Alien Registration Number), enter it here.
DO NOT ENTER INFORMATION IN THE FOLLOWING FIELDS:
ORI
OCA
ANY OTHER FIELD MARKED “LEAVE BLANK”
CYFD Background Check Unit |
07/30/2010 |
APPLICANT WRITTEN STATEMENT
INSTRUCTIONS: Use additional sheets as necessary. All questions must be answered completely and to the best of your knowledge. If you are applying for “Employment in a Licensed Childcare Home,” all adult household members (age 18 and over) must fill out their own Applicant Written Statement and provide fingerprint card and the required fee. Please print legibly. Answers left blank, or a response of “N/A” may result in the rejection of the application.
Full Name (include birth name, married name(s), nick names, and aliases. Do not use initials). |
|
||
Date of Birth (month, day, year) |
Place of Birth (city, state, country) |
Social Security Number |
Primary Language |
______/ ______ / __________ |
___________________, ______/_______ |
_______ - _____ - __________ |
_________________________ |
Current Physical Address
_______________________________
Address
_______________________________
Address (optional)
_______________, _______________
City |
State |
Zip |
Mailing Address (if different from physical)
_______________________________
Address
_______________________________
Address (optional)
_______________, _______________
City |
State |
Zip |
Contact Information
_______________________________
Primary Phone Number
_______________________________
Secondary Phone Number (optional)
_______________________________
Previous Address/Addresses (past ten years, most recent first, and include number, street, city, state, zip code.)
If you need more space, use a separate sheet of paper.
_______________________________ |
_______________________________ |
_______________________________ |
||||||
Address |
|
|
Address |
|
|
Address |
|
|
_______________________________ |
_______________________________ |
_______________________________ |
||||||
Address (optional) |
|
|
Address (optional) |
|
|
Address (optional) |
|
|
_______________, _______________ |
_______________, _______________ |
_______________, _______________ |
||||||
City |
State |
Zip |
City |
State |
Zip |
City |
State |
Zip |
Current Spouse/Significant Other |
|
|
|
|
|
|
________________________________________________ |
______/ ______ / __________ |
_____ |
|
__ - _____ - __________ |
||
First |
Middle |
Last |
Date of Birth(month, day, year) |
|
Social Security Number |
|
Full Name(s) and Date(s) of Birth of: Birth Children, Adopted Children, Foster Children, and other Children who have lived in your household(s) within the past ten years (If you need more space, use a separate sheet of paper)
First Name |
|
Middle Name |
Last Name |
|
Date of Birth (month, day, year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
Current Marital Status (circle one): Single |
Married |
Separated |
Divorced |
Widowed |
|
|
Full Name(s) and Date(s) of Birth of all Adults who have previously lived with you (within the past ten years) (If you need more space, use a separate sheet of paper)
|
First Name |
Middle Name |
Last Name |
Date of Birth (month, day, year) |
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
CYFD Background Check Unit |
|
|
|
07/30/2010 |
|
Full Name(s) and Date(s) of Birth of all Adults who are currently living with you (If you need more space, use a separate sheet of paper)
First Name |
Middle Name |
Last Name |
Date of Birth (month, day, year) |
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
Names and Places of School(s) attended, along with graduation dates (High School, University, College, and Vocational Training) (If you need more space, use a separate sheet of paper)
Name of School
Location of School
Graduation Date
Type (high school, college, etc.)
Employment History (list all dates and places of employment from age 18 to date - explain breaks in employment) (If you need more space, use a separate sheet of paper)
Employer
Start Date
End Date
Explain Break in Employment
IF YOU DO NOT UNDERSTAND THESE QUESTIONS, PLEASE SEEK GUIDANCE BEFORE ANSWERING THEM!
Have you ever been involved in a CYFD investigation of abuse or neglect of children or adults as the alleged perpetrator or household member? If so, provide the dates of all such investigations and the outcome of those investigations. NOTE: Failure to provide this information may lead to denial of your application.
_____ Yes, I have been involved in a CYFD (or other protective service agency) investigation of abuse or neglect of children or adults as the alleged
perpetrator or household member (Provide details).
_____ No, I have never been involved in a CYFD (or other protective service agency) investigation of abuse or neglect of children or adults as the alleged
perpetrator or household member.
Have you ever been charged with, arrested for, or convicted of a crime? NOTE: Failure to provide this information may lead to denial of your application.
_____ Yes, I have been charged with, arrested for, or convicted of a crime (Provide an explanation and disposition).
_____ No, I have never been charged with, arrested for, or convicted of a crime. |
|
|||||
Under penalty of perjury, I ____________________ |
|
|
__________ certify the above statements to be true and complete to the best |
|||
of my knowledge. |
|
|
|
|
|
|
SIGNATURE: ________________________ |
|
|
___ |
_______ |
DATE: _____________ |
|
|
|
|
|
|
|
|
CYFD. Background Check Unit. Applicant Written Statement. 07/30/2010. Page 2
EMPLOYER STATEMENT
I, ____________________________, authorized representative of _______________________, hereby
(NAME OF HR REP OR DIRECTOR)(NAME OF FACILITY)
attest that __________________________, is an applicant for employment, an employee, contractor or
(NAME OF APPLICANT)
volunteer with _____________________. This applicant, employee, contractor or volunteer requires a
(NAME OF FACILITY)
CYFD background check pursuant to 8.8.3 NMAC and has direct care responsibilities or potential unsupervised access to care recipients.
I understand that by signing this statement, ____________________________ waives any claim that
(NAME OF FACILITY)
this applicant, employee, contractor or volunteer does not have direct care responsibilities or does not have potential unsupervised access to care recipients in the event that he/she is determined to be an unreasonable risk and denied background check eligibility.
____________________________________
NAME OF EMPLOYER REPRESENTATIVE
____________________________________
TITLE
____________________________________
PHONE NUMBER
____________________________________
DATE
Disposition Request Information Sheet
CYFD is requesting disposition because some types of convictions can result in denial of a background check clearance. Disposition means outcome. CYFD wants to know the final outcome of the arrest.
Where to find disposition
Disposition can often be found at the courts in the county where you were arrested. You can also contact the agency that arrested you, or contact the attorney who represented you, if you had one.
Phone numbers for the Courts, Police Departments, and Attorneys can generally be found in the phone book, in the Government and/or Yellow pages. Out of state information might be found on the internet.
Acceptable forms of disposition
Dispositional information can be found in documents called:
Judgment and Sentence
Plea and Disposition Agreement
Nolle Prosequi
Certificate of Conviction
If you are unsure which of the forms contains your disposition, ask the Court clerk for help.
We will not accept
Clerk’s Certificates marked “No Felony Convictions”
Documentation from the arresting agency marked “No Record Found”
An explanation of the arrest from your attorney.
Please call our office at (505)
Disposition must be received no later than 15 days after the date of the request. It is your responsibility to provide this information to CYFD. This sheet is for informational purposes only. Your search for disposition should not be limited to the ideas presented here.
Rehabilitation Petition Information Sheet
What is a rehabilitation petition?
A rehabilitation petition is an opportunity for the applicant to submit information regarding a criminal or protective services history that might otherwise result in a determination of unreasonable risk.
Why am I being asked to submit this information?
AS Background Check Unit has determined that an arrest or referral in your past might indicate that you are an unreasonable risk.
How do I submit a rehabilitation petition?
If you are required to submit a rehabilitation petition, AS Background Check Unit will mail you a request.
What should I include in a rehabilitation petition?
1.A statement telling AS Background Check Unit what steps you have taken to assure that the event(s) we inquire about will not happen again.
2.Do include:
a.A specific description of what actions you have taken subsequent to any events revealed by the background check to reduce the risk that the same or a similar circumstance will
b.Specific examples that prove rehabilitation by clear and convincing evidence
3.Do not include:
a.Court documents, certificates, character references, or other collateral information UNLESS it is used to prove your statements
b.Court documents, certificates, character references, or other collateral information instead of a statement
What if I have questions?
If you have questions regarding the rehabilitation petition, contact the AS Background Check Unit at
How will I know if you accept the petition?
Please allow AS Background Check Unit at least 7 working days to review the information you submit; you will receive a response in the mail.
What if I do not want to do the petition?
Failure to return the petition to us within fifteen days of the mail date of the letter, will result in denial of the application, in accordance with 8.8.3.10(C) NMAC, which states: “If there is a need for any further information from an applicant at any stage of the process, the department shall request the information in writing from the applicant. If the department does not receive the requested information within fifteen calendar days of the date of the request the department shall deny the application.”
What if I need more than 15 days to do the petition?
You must contact the AS Background Check Unit, in writing, to secure an extension. Requests for extension can be mailed, faxed, or mailed electronically to:
FAX: |
|
|
|
ADDRESS: CYFD / AS / BCU |
|
|
|
PO DRAWER 5160 |
|
|
|
SANTA |
FE |
NM |
FREQUENTLY ASKED QUESTIONS
Q:What is the applicant written statement? Why do I have to fill it out? Do I have to answer all of the questions?
A:The applicant written statement is used to further identify you, in the event we encounter a person who has the same name as you. If you are applying for “Employment in a Licensed Childcare Home,” all household members over the age of 18 must complete the applicant written statement. You must answer all of the questions.
Q:How long does the process take?
A:Please allow CYFD 30 days to process your application. If you do not have an answer 30 days after we receive the application, please call to determine what the status is. We can be reached at (505)
Q:What if I have a criminal history? What is a disposition?
A:Disposition means outcome. In the event that you have been arrested or convicted of a crime, CYFD must have disposition because some types of convictions can affect the outcome of your application. CYFD wants to know the final outcome of the arrest and/or conviction. Please see the disposition information sheet for more information.
Q:What if I get a letter that says I cannot provide care?
A:The letter will contain information on how to file an appeal or instruct you to gather more information in order to continue processing your background check.
TITLE 8 SOCIAL SERVICES
CHAPTER 8 CHILDREN, YOUTH AND FAMILIES GENERAL PROVISIONS PART 3 GOVERNING BACKGROUND CHECKS AND EMPLOYMENT HISTORY
VERIFICATION
8.8.3.1ISSUING AGENCY: Children, Youth and Families Department [8.8.3.1 NMAC - Rp, 8.8.3.1 NMAC, 03/31/06]
8.8.3.2SCOPE: This rule has general applicability to operators, volunteers, including student interns, staff and employees, and prospective operators, staff and employees, of child- care facilities, including every facility, CYFD contractor, program receiving CYFD funding or reimbursement, or other program that has or could have primary custody of children for twenty hours or more per week, juvenile treatment facilities, and direct providers of care for children in including, but not limited to the following settings: Children’s behavioral health services and licensed and registered child care, including shelter care.
[8.8.3.2 NMAC - Rp, 8.8.3.2 NMAC, 03/31/06; A, 07/31/09]
8.8.3.3STATUTORY AUTHORITY: The statutory authority for these regulations is contained in the Criminal Offender Employment Act, Section
[8.8.3.3 NMAC - Rp, 8.8.3.3 NMAC, 03/31/06]
8.8.3.4DURATION: Permanent
[8.8.3.4 NMAC - Rp, 8.8.3.4 NMAC, 03/31/06]
8.8.3.5EFFECTIVE DATE: March 31, 2006, unless a later date is cited at the end of
a section.
[8.8.3.5 NMAC - Rp, 8.8.3.5 NMAC, 03/31/06]
8.8.3.6OBJECTIVE:
A.The purpose of these regulations is to set out general provisions regarding background checks and employment history verification required by the children, youth and families department.
B.Background checks are conducted in order to identify information in applicants’ backgrounds bearing on whether they are eligible to provide services in settings to which these regulations apply.
C.Abuse and neglect screens are conducted by licensing authority staff in order to identify those persons who pose a continuing threat of abuse or neglect to minors or adults in settings to which these regulations apply.
[8.8.3.6 NMAC - Rp, 8.8.3.6 NMAC, 03/31/06; A 07/31/09]
8.8.3.7DEFINITIONS:
A.ADMINISTRATIVE REVIEW means an informal process of reviewing a decision that may include an informal conference or hearing or a review of written records.
B.ADMINISTRATOR means the adult in charge of the
C.ADULT means a person who has a chronological age of 18 years or older, except for persons under medicaid certification as set forth in Subsection I below.
D.APPEAL means a review of a determination made by the children, youth and families department, which may include an administrative review.
E.APPLICANT means any person who is required to obtain a background check under these rules and NMSA 1978, Section
F.ARREST means notice from a law enforcement agency about an alleged violation of law.
G.BACKGROUND CHECK means a screen of the department’s information databases, state and federal criminal records and any other reasonably reliable information about an applicant.
H.CARE RECIPIENT means any person under the care of a licensee.
I.CHILD means a person who has a chronological age of less than 18 years, and persons under applicable medicaid certification up to the age of 21 years.
J.CONDITIONAL EMPLOYMENT means a period of employment status for a new applicant prior to the licensing authority’s final disposition of the applicant’s background check.
K.CRIMINAL HISTORY means information possessed by law enforcement agencies of arrests, indictments, or other formal charges, as well as dispositions arising from these charges.
L.DIRECT, PHYSICAL SUPERVISION means continuous visual contact or live video observation by a direct provider of care who has been found eligible by a background check of an applicant during periods when the applicant is in immediate physical proximity to care recipients.
M.DIRECT PROVIDER OF CARE means any individual who, as a result of employment or, contractual service or volunteer service has direct care responsibilities or potential unsupervised physical access to any care recipient in the settings to which these regulations apply.
N.EMPLOYMENT HISTORY means a written summary of the most recent three- year period of employment with names, addresses and telephone numbers of employers, including dates of employment, stated reasons for leaving employment, and dates of all periods of unemployment with stated reasons for periods of unemployment, and verifying references.
O.LICENSED means authorized to operate by the children, youth and families department by issuance of an operator’s license or certification certificate.
P.LICENSEE means the holder of, or applicant for, a license, certification, or registration pursuant to 7.20.11 NMAC, 7.20.12 NMAC, 8.16.2 NMAC, 7.8.3 NMAC; 8.17.2 NMAC.
Q.LICENSING AUTHORITY means the children, youth and families department.
R.MORAL TURPITUDE means an intentional crime that is wanton, base, vile or depraved and contrary to the accepted rules of morality and duties of a person within society. In addition, because of the high risk of injury or death created by, and the universal condemnation of the act of driving while intoxicated, a crime of moral turpitude includes a second or subsequent conviction for driving while intoxicated or any crime involving the use of a motor vehicle, the elements of which are substantially the same as driving while
intoxicated. The record name of the second conviction shall not be controlling; any conviction subsequent to an initial one may be considered a second conviction.
S.RELEVANT CONVICTION means a plea, judgment or verdict of guilty, no contest, nolo contendere, conditional plea of guilty, or any other plea that would result in a conviction for a crime in a court of law in New Mexico or any other state. The term RELEVANT CONVICTION also includes decrees adjudicating juveniles as serious youthful offenders or youthful offenders, or convictions of children who are tried as adults for their offenses. Successful or pending completion of a conditional discharge under NMSA 1978, Section
T.UNREASONABLE RISK means the quantum of risk that a reasonable person would be unwilling to take with the safety or welfare of care recipients.
[8.8.3.7 NMAC - Rp, 8.8.3.7 NMAC, 03/31/06; A, 07/31/09]
8.8.3.8APPLICABILITY: These regulations apply to all licensees and direct providers of care in the following settings:
A.behavior management skills development;
B.case management services;
C.group home services;
D.day treatment services;
E.residential treatment services;
F.treatment foster care services agency staff;
Glicensed child care homes;
H.licensed child care centers;
I.registered child care homes;
J.licensed shelter care;
K.licensed before and after school care;
L.
M.comprehensive community support services;
N.CYFD contractors and any other programs receiving CYFD funding or reimbursement.
[8.8.3.8 NMAC - Rp, 8.8.3.8 NMAC, 03/31/06; A, 07/31/09]
8.8.3.9
A.These regulations do not apply to the following settings, except when otherwise required by applicable Certification Requirements for Child and Adolescent Mental Health Services 7.20.11 NMAC or to the extent that such a program receives funding or reimbursement from CYFD:
(1)hospitals or infirmaries;
(2)intermediate care facilities;
(3)children’s psychiatric centers;
(4)home health agencies;
(5)diagnostic and treatment centers;
(6)unlicensed or unregistered child care homes.
B.These regulations do not apply to the following adults:
(1)treatment foster care parents;
(2)relative care providers who are not otherwise required to be licensed or
registered;
(3)foster grandparent volunteers;
(4)volunteer parents of an enrolled child if the parent is under direct physical
supervision;
(5)all other volunteers at a licensed or registered facility if the volunteer spends less than six hours per week at the facility, is under direct physical supervision, and is not counted in the facility ratio.
[8.8.3.9 NMAC - Rp, 8.8.3.9 NMAC, 03/31/06; A, 07/31/09]
8.8.3.10COMPLIANCE:
A.Compliance with these regulations is a condition of licensure, registration, certification or renewal, or continuation of same.
B.The licensee is required to:
(1)submit two completed
(2)submit the
fee;
(3)submit the name, address, date of birth and any aliases of the direct care provider for a child abuse and neglect screen;
(4)verify the employment history of any potential direct provider of care the verification shall include contacting references and prior employers/agencies to elicit information regarding the reason for leaving prior employment or service; the verification shall
be documented and available for review by the licensing authority; EXCEPTION: Verification of employment history is not required for registered home providers, child care homes licensed for six (6) or fewer children, or relative care providers;
(5)submit an adult household member written statement form for each adult household member in a registered home setting in order to conduct criminal history and child abuse and neglect screens on such household members; an adult household member is an adult living in the household or an adult that spends a significant amount of time in the home;
(6)provide such other information department staff determines to be necessary;
and
(7)maintain documentation of all applications, correspondence and clearances relating to the background checks required; in the event that the licensee does not have a copy of an applicant’s clearance documentation and upon receipt of a written request for a copy, the
department may issue duplicate clearance documentation to the original licensee; the request for duplicate clearance documentation must be made within one year of the applicant’s clearance date.
C.If there is a need for any further information from an applicant at any stage of the process, the department shall request the information in writing from the applicant. If the department does not receive the requested information within fifteen calendar days of the date of the request, the department shall deny the application.
[8.8.3.10 NMAC - Rp, 8.8.3.10 NMAC, 03/31/06; A, 07/31/09]
8.8.3.11COMPLIANCE EXCEPTIONS:
A.An applicant may not begin providing services prior to obtaining a background eligibility unless all of the following requirements are met:
(1)the licensee may not be operating under a corrective action plan (childcare), sanctions, or other form of licensing disciplinary serious violations;
(2)until receiving background eligibility the applicant shall at all times be under direct physical supervision; this provision does not apply to registered child care home applicants;
(3)by the end of the next day after the applicant begins providing services, the applicant shall send the licensing authority a completed application form and fingerprint cards;
(4)within fifteen days after the applicant begins providing services, the applicant shall provide the licensing authority with all information necessary for the background check; and
(5)no more than 45 days shall have passed since the date of the initial application unless the department documents good cause shown for an extension.
B.If a direct provider has a break in employment or transfers employment more than 180 days after the date of an eligibility letter from the licensing authority the direct care provider must
(1)the direct provider submits a statement swearing under penalty of perjury that he or she has not been arrested or charged with any crimes, has not been an alleged perpetrator of abuse or neglect and has not been a respondent in a domestic violence petition;
(2)the direct care provider submits an application that describes the prior and subsequent places of employment, registration or certification with sufficient detail to allow the licensing authority to determine if further background checks or a new application is necessary; and
(3)the licensing authority determines within 15 days that the direct care provider’s prior background check is sufficient for the employment or position the direct care provider is going to take.
[8.8.3.11 NMAC - Rp, 8.8.3.11 NMAC, 03/31/06; A, 04/15/08; A, 07/31/09]
8.8.3.12PROHIBITIONS:
A.Any licensee who violates these regulations is subject to revocation, suspension, sanctions, or denial of licensure, certification, or registration.
B.Licensure, certification, or registration is subject to receipt by the licensing authority of a satisfactory background check for the licensee or the licensee’s administrator.
C.Except as provided in 8.8.3.13 NMAC below, licensure, certification or registration may not be granted by the licensing authority if a background check of the licensee or the licensee’s administrator reveals an unreasonable risk.
D.A licensee may not retain employment, volunteer service or contract with any direct provider of care for whom a background check reveals an unreasonable risk. The department shall deliver one copy of the notice of unreasonable risk to the facility or program by U.S. mail and to the appropriate licensing staff at the department by facsimile transmission or hand delivery.
E.A licensee shall be in violation of these regulations if it retains a direct provider of care for more than ten working days following the mailing of a notice of background check denial for failure to respond by the licensing authority.
F.A licensee shall be in violation of these regulations if it retains any direct provider of care inconsistent with Subsection A of 8.8.3.11 NMAC.
G.A licensee shall be in violation of these regulations if it hires, contracts with, uses in volunteer service, or retains any direct provider of care for whom information received from any source including the direct provider of care, indicates the provider of care poses an unreasonable risk to the department or to care recipients.
H.Any firm, person, corporation, individual or other entity that violates this section shall be subject to appropriate disciplinary action up to and including immediate emergency revocation of license or registration pursuant to the regulations applicable to that entity.
[8.8.3.12 NMAC - Rp, 8.8.3.12 NMAC, 03/31/06; A, 07/31/09]
8.8.3.13ARRESTS, CONVICTIONS AND REFERRALS:
A.For the purpose of these regulations, the following information shall result in a conclusion that the applicant is an unreasonable risk:
(1)a conviction for a felony or a misdemeanor involving moral turpitude and the criminal conviction directly relates to whether the applicant can provide a safe, responsible and morally positive setting for care recipients;
(2)a conviction for a felony or a misdemeanor involving moral turpitude and the criminal conviction does not directly relate to whether the applicant can provide a safe, responsible and morally positive setting for care recipients if the department determines that the applicant so convicted has not been sufficiently rehabilitated;
(3)a conviction, regardless of the degree of the crime or the date of the conviction, of trafficking in controlled substances, criminal sexual penetration or related sexual offenses or child abuse; or
(4)a substantiated referral, regardless of the date, for sexual abuse or for neglect characterized by a failure to protect against sexual abuse.
B.A disqualifying conviction may be proven by:
(1)a copy of the judgment of conviction from the court;
(2)a copy of a plea agreement filed in court in which a defendant admits guilt;
(3)a copy of a report from the federal bureau of investigation, criminal information services division, or the national criminal information center, indicating a conviction;
(4)a copy of a report from the state of New Mexico, department of public safety, or any other agency of any state or the federal government indicating a conviction;
(5)any writing by the applicant indicating that such person has been convicted of the disqualifying offense, provided, however, that if this is the sole basis for denial, the applicant shall be given an opportunity to show that the applicant has successfully completed or is pending completion of a conditional discharge for the disqualifying conviction.
C.If a background check shows pending charges for a felony offense, any misdemeanor offense involving domestic violence or child abuse, an arrest but no disposition for any such crime, or a pending referral with the department, there shall be a determination of unreasonable risk. An arrest or criminal charge for any felony offense or for any misdemeanor offense involving domestic violence or child abuse shall result in the immediate suspension of the applicant’s background check status until such time as the charges are disposed of. It is the duty of the administrator of a facility or the licensee, upon learning of any such arrest or criminal charge, to notify the licensing authority immediately. A suspension of background check status shall have the same effect as a determination of unreasonable risk until the charges are disposed of. If an arrest or criminal charge results in a conviction, the applicant may reapply for background check eligibility and shall be subject to all applicable criminal records check provisions and may be determined to be an unreasonable risk. If an arrest or criminal charge results in an acquittal, conditional discharge, suspension of proceedings based on participation in a
D.If a background check shows that an applicant is wanted for any offense by any law enforcement agency due to a warrant having been issued, or if the applicant is shown to have failed to appear for any pending criminal court proceeding, there shall be a determination of unreasonable risk. If such information shall be reported to the licensing authority after an initial determination that the applicant is eligible, the applicant’s background check status shall be suspended until such time as the matter is disposed of. After the matter has been disposed of, the applicant shall be subject to all of the background check provisions set forth in Subsections A, B, and C above.
[8.8.3.13 NMAC - Rp, 8.8.3.13 NMAC, 03/31/06; A, 07/31/09]
8.8.3.14UNREASONABLE RISK:
A.The department may, in its discretion, weigh the evidence about an applicant to determine whether the applicant poses an unreasonable risk to the department or care recipients. The department may also consult with legal staff, treatment, assessment or other professionals in the process of determining whether the cumulative weight of credible evidence establishes unreasonable risk.
B.In determining whether an applicant poses an unreasonable risk, the department need not limit its reliance on formal convictions or substantiated referrals, but nonetheless must only rely on evidence with indicia of reliability such as:
(1)reliable disclosures by the applicant or a victim of abuse or neglect;
(2)domestic violence orders that allowed an applicant notice and opportunity to be heard and that prohibits or prohibited them from injuring, harassing or contacting another;
(3)circumstances indicating the applicant is or has been a victim of domestic
violence;
(4)child or adult protection investigative evidence that indicates a likelihood that an applicant engaged in inappropriate conduct but there were reasons other than the credibility of the evidence to not substantiate; or
(5)any other evidence with similar indicia of reliability.
[8.8.3.14 NMAC - N, 03/31/06; A, 07/31/09]
8.8.3.15REHABILITATION PETITION: Any applicant whom the department concludes is an unreasonable risk on any basis other than those described at Paragraphs (3) or (4) of Subsection A of 8.8.3.13 NMAC, may submit to the department a rehabilitation petition describing with specificity all information that tends to demonstrate that the applicant is not an unreasonable risk. The petition may include, but need not be limited to, a description of what actions the applicant has taken subsequent to any events revealed by the background check to reduce the risk that the same or a similar circumstance will recur.
[8.8.3.15 NMAC - N, 03/31/06]
8.8.3.16APPEAL RIGHTS:
A.Any licensee who is denied licensure, certification, or registration or is sanctioned pursuant to these regulations or a previously cleared direct provider of care whose eligibility has been suspended may appeal that decision to the children, youth and families department. If a licensee or a previously cleared direct provider of care alleges facts in good faith that demonstrate a conclusion of unreasonable risk will substantially affect a present vested right such as current employment or other similar currently vested rights the licensee shall be entitled to a hearing. The request for appeal shall be in writing and the party requesting the appeal shall cause the department to receive it within fifteen days of the date of the department’s written notice of a determination of unreasonable risk.
B.Any direct provider of care who is found ineligible after completion of background check may request an administrative review from the children, youth and families department. The request for an administrative review shall be in writing and the party requesting the appeal shall cause the department to receive it within fifteen days of the date of the department’s written notice of a determination of unreasonable risk.
C.The administrative review shall be completed by a review of the record by a hearing officer designated by the cabinet secretary. The hearing officer’s review is limited to:
(1) whether the licensing authority’s conclusion of unreasonable risk is supported by any section of these regulations; and (2) whether the applicant has been erroneously identified as a person with a relevant conviction or substantiated referral. The review will be completed on the record presented to the hearing officer and includes the applicant’s written request for an administrative review and other relevant evidence provided by the applicant. The hearing officer conducts the administrative review and submits a recommendation to the cabinet secretary no later than 60 days after the date the request for administrative review is received unless the department and the applicant agree otherwise. The appeal that is a hearing under this section shall be pursuant to the department’s administrative hearing regulations at 8.8.4 NMAC.
[8.8.3.16 NMAC - Rp, 8.8.3.15 NMAC 03/31/06; A, 07/31/09]
HISTORY OF 8.8.3 NMAC:
HED
History of Repealed Material:
HED
8.8.3NMAC, Governing Criminal Records Checks and Employment History Verification, filed 7/30/2001 - Repealed effective 3/29/2002.
8.8.3NMAC, Governing Criminal Records Checks and Employment History Verification, filed 3/15/2002 - Repealed effective 10/30/03.
8.8.3NMAC, Governing Background Checks and Employment History Verification, filed 10/16/2003 - Repealed effective 3/31/2006.