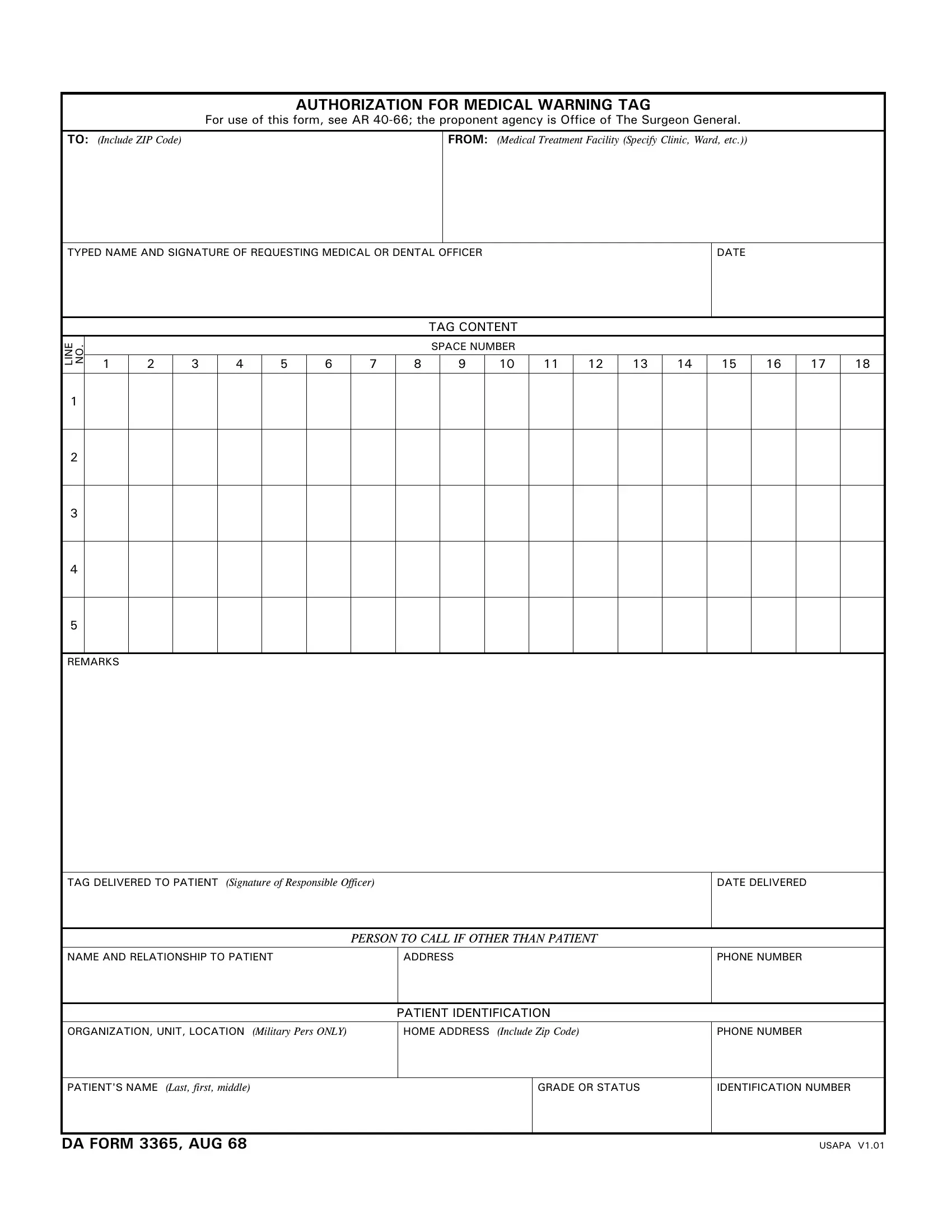
At its core, the DA Form 3365, known as the Authorization for Medical Warning Tag, plays a critical role within the framework of military health services. This comprehensive document, governed under the regulatory guidelines of AR 40-66 and overseen by the Office of The Surgeon General, is a testament to the meticulously organized process of managing health-related alerts within the armed forces. The form serves as a communication bridge between medical professionals within military treatment facilities—including clinics and wards—and their patients, ensuring that crucial medical warnings are formally documented and appropriately conveyed. Details such as the patient’s identification, the specific content of the medical warning tag, and the responsible officer’s acknowledgment of the tag's delivery to the patient are meticulously captured. This form not only facilitates the exchange and recording of important medical information but also details instructions for contacting individuals related to the patient, should the need arise. By implementing such a protocol, the DA Form 3365 emblematically upholds the military's high standard of care, demonstrating a structured commitment to the health and safety of its personnel.
| Question | Answer |
|---|---|
| Form Name | Da 3365 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Pers, V1, da form 3365, form |
AUTHORIZATION FOR MEDICAL WARNING TAG
For use of this form, see AR
TO: (Include ZIP Code) |
FROM: (Medical Treatment Facility (Specify Clinic, Ward, etc.)) |
|
|
TYPED NAME AND SIGNATURE OF REQUESTING MEDICAL OR DENTAL OFFICER
DATE
LINE NO.
TAG CONTENT
SPACE NUMBER
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
1
2
3
4
5
REMARKS
TAG DELIVERED TO PATIENT (Signature of Responsible Officer)
DATE DELIVERED
PERSON TO CALL IF OTHER THAN PATIENT
NAME AND RELATIONSHIP TO PATIENT
ADDRESS
PHONE NUMBER
PATIENT IDENTIFICATION
ORGANIZATION, UNIT, LOCATION (Military Pers ONLY) |
HOME ADDRESS (Include Zip Code) |
PHONE NUMBER |
|
|
|
|
|
PATIENT'S NAME (Last, first, middle) |
|
GRADE OR STATUS |
IDENTIFICATION NUMBER |
|
|
|
|
DA FORM 3365, AUG 68
USAPA V1.01