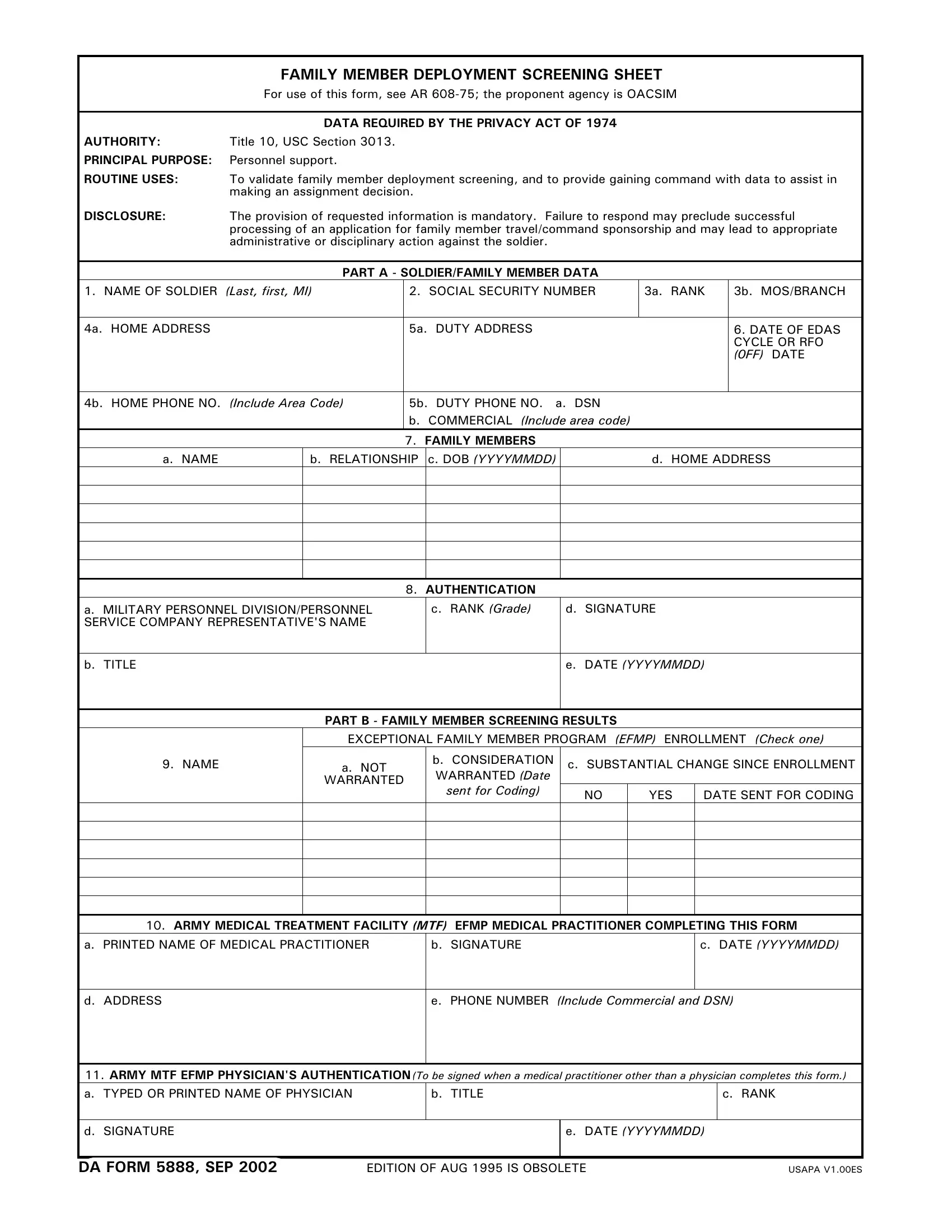
Understanding the DA Form 5888, the Family Member Deployment Screening Sheet, is crucial for military personnel navigating the intricacies of deployment and ensuring their family's needs are addressed. This form is integral to the Army's process, serving multiple purposes including validating family member deployment screening and aiding in assignment decisions by providing essential data to the gaining command. Mandated by the Privacy Act of 1974, it demands a comprehensive collection of soldier and family member data, underlying its significance in maintaining personnel support. Failure to accurately complete the form can have serious ramifications, potentially hindering the processing of applications for family member travel or command sponsorship. With sections ranging from soldier/family member data to detailed screening results, the form meticulously captures information vital for enrollment in the Exceptional Family Member Program (EFMP), ensuring that families with special needs are given the consideration they require. As such, the DA Form 5888 stands as a cornerstone document, underscoring the Army's commitment to the well-being of its servicemen and women's families, particularly as they face the challenges of deployment.
| Question | Answer |
|---|---|
| Form Name | DA 5888 Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 1 |
| Avg. time to fill out | 27 sec |
| Other names | form 5888, da5888, da 5888, fillable da 5888 |
|
FAMILY MEMBER DEPLOYMENT SCREENING SHEET |
|
For use of this form, see AR |
|
|
|
DATA REQUIRED BY THE PRIVACY ACT OF 1974 |
AUTHORITY: |
Title 10, USC Section 3013. |
PRINCIPAL PURPOSE: |
Personnel support. |
ROUTINE USES: |
To validate family member deployment screening, and to provide gaining command with data to assist in |
|
making an assignment decision. |
DISCLOSURE: |
The provision of requested information is mandatory. Failure to respond may preclude successful |
|
processing of an application for family member travel/command sponsorship and may lead to appropriate |
|
administrative or disciplinary action against the soldier. |
PART A - SOLDIER/FAMILY MEMBER DATA
1. NAME OF SOLDIER (Last, first, MI) |
2. SOCIAL SECURITY NUMBER |
3a. RANK |
3b. MOS/BRANCH |
|
|
|
|
4a. HOME ADDRESS |
5a. DUTY ADDRESS |
|
6. DATE OF EDAS |
|
|
|
CYCLE OR RFO |
|
|
|
(0FF) DATE |
|
|
|
|
4b. HOME PHONE NO. (Include Area Code) |
5b. DUTY PHONE NO. a. DSN |
|
|
b.COMMERCIAL (Include area code)
7.FAMILY MEMBERS
a. NAME
b. RELATIONSHIP c. DOB (YYYYMMDD)
d. HOME ADDRESS
8. |
AUTHENTICATION |
|
a. MILITARY PERSONNEL DIVISION/PERSONNEL |
c. RANK (Grade) |
d. SIGNATURE |
SERVICE COMPANY REPRESENTATIVE'S NAME |
|
|
|
|
|
b. TITLE
e.DATE (YYYYMMDD)
PART B - FAMILY MEMBER SCREENING RESULTS
9. NAME
EXCEPTIONAL FAMILY MEMBER PROGRAM (EFMP) ENROLLMENT (Check one)
a. NOT |
b. CONSIDERATION |
c. SUBSTANTIAL CHANGE SINCE ENROLLMENT |
||
WARRANTED (Date |
|
|
|
|
WARRANTED |
|
|
|
|
sent for Coding) |
|
|
|
|
|
NO |
YES |
DATE SENT FOR CODING |
|
|
|
|||
|
|
|
|
|
10. ARMY MEDICAL TREATMENT FACILITY (MTF) EFMP MEDICAL PRACTITIONER COMPLETING THIS FORM
a. PRINTED NAME OF MEDICAL PRACTITIONER
b. SIGNATURE
c.DATE (YYYYMMDD)
d. ADDRESS
e. PHONE NUMBER (Include Commercial and DSN)
11. ARMY MTF EFMP PHYSICIAN'S AUTHENTICATION(To be signed when a medical practitioner other than a physician completes this form.)
a. TYPED OR PRINTED NAME OF PHYSICIAN
b. TITLE
c. RANK
d. SIGNATURE
e.DATE (YYYYMMDD)
DA FORM 5888, SEP 2002 |
EDITION OF AUG 1995 IS OBSOLETE |
USAPA V1.00ES |