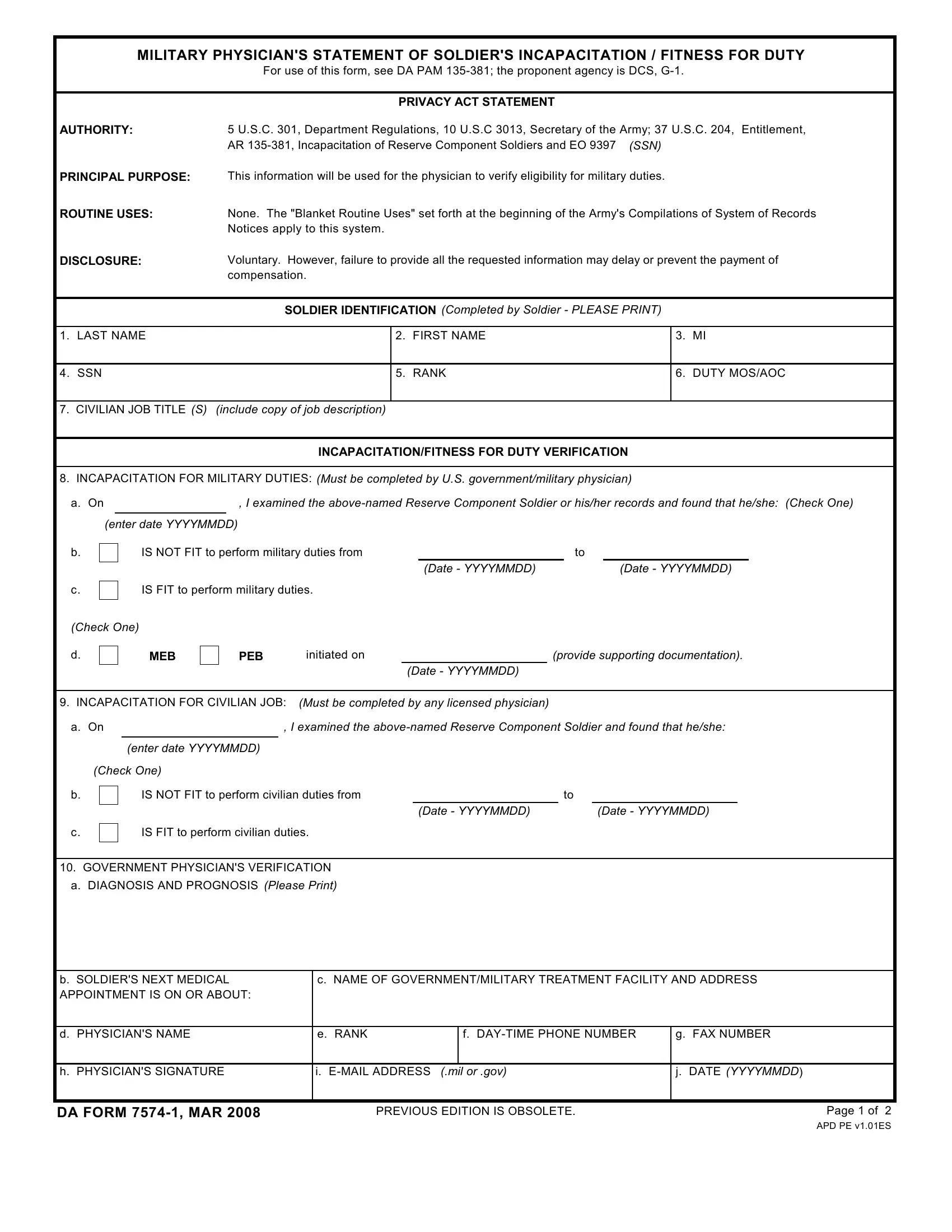
Understanding the critical role of the DA Form 7574-1, officially known as the Military Physician's Statement of Soldier's Incapacitation/Fitness for Duty, sheds light on the procedural aspects of managing the health and duty status of Reserve Component Soldiers within the U.S. military. This essential document serves a dual-purpose, allowing military physicians to formally assess and document a soldier's ability to perform military and civilian duties. Governed by DA PAM 135-381 and underpinned by various legal authorities and privacy considerations, it ensures that a structured and standardized approach is adopted for evaluating a soldier's fitness. Key components of the form include identifying soldier information, a section for incapacitation/fitness for duty verification by a U.S. government or military physician, and detailed instructions for the physician completing the form, including diagnosis, prognosis, and follow-up details. Its proper use is not only vital for the soldier's welfare but also crucial in the administrative and operational readiness of the military unit involved, demonstrating the form's significance in bridging healthcare assessments with military duty considerations.
| Question | Answer |
|---|---|
| Form Name | Da Form 7574 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 7574 1, da 7574 fillable blank, mail 7574 1 online, form 7574 |
MILITARY PHYSICIAN'S STATEMENT OF SOLDIER'S INCAPACITATION / FITNESS FOR DUTY
For use of this form, see DA PAM
AUTHORITY:
PRINCIPAL PURPOSE:
ROUTINE USES:
DISCLOSURE:
PRIVACY ACT STATEMENT
5 U.S.C. 301, Department Regulations, 10 U.S.C 3013, Secretary of the Army; 37 U.S.C. 204, Entitlement, AR
This information will be used for the physician to verify eligibility for military duties.
None. The "Blanket Routine Uses" set forth at the beginning of the Army's Compilations of System of Records Notices apply to this system.
Voluntary. However, failure to provide all the requested information may delay or prevent the payment of compensation.
SOLDIER IDENTIFICATION (Completed by Soldier - PLEASE PRINT)
1. LAST NAME
2. FIRST NAME
3. MI
4. SSN
5. RANK
6. DUTY MOS/AOC
7.CIVILIAN JOB TITLE (S) (include copy of job description)
INCAPACITATION/FITNESS FOR DUTY VERIFICATION
8.INCAPACITATION FOR MILITARY DUTIES: (Must be completed by U.S. government/military physician)
a. On |
|
, I examined the |
|
|
|
(enter date YYYYMMDD)
b.
IS NOT FIT to perform military duties from |
to |
||
|
(Date - YYYYMMDD) |
|
(Date - YYYYMMDD) |
c.
IS FIT to perform military duties.
(Check One)
d. |
MEB |
PEB |
initiated on |
|
(provide supporting documentation). |
|
|
(Date - YYYYMMDD) |
|
9.INCAPACITATION FOR CIVILIAN JOB: (Must be completed by any licensed physician)
a. On |
|
, I examined the |
|
|
|
(enter date YYYYMMDD)
(Check One)
b.
c.
IS NOT FIT to perform civilian duties from |
to |
||
|
(Date - YYYYMMDD) |
|
(Date - YYYYMMDD) |
IS FIT to perform civilian duties. |
|
|
|
10.GOVERNMENT PHYSICIAN'S VERIFICATION a. DIAGNOSIS AND PROGNOSIS (Please Print)
b.SOLDIER'S NEXT MEDICAL APPOINTMENT IS ON OR ABOUT:
c. NAME OF GOVERNMENT/MILITARY TREATMENT FACILITY AND ADDRESS
d. PHYSICIAN'S NAME
e. RANK
f.
g. FAX NUMBER
h. PHYSICIAN'S SIGNATURE
i.
j.DATE (YYYYMMDD)
DA FORM |
PREVIOUS EDITION IS OBSOLETE. |
Page 1 of 2 |
APD PE v1.01ES
MILITARY PHYSICIAN'S STATEMENT OF SOLDIER'S
INCAPACITATION/FITNESS FOR DUTY
INSTRUCTION SHEET
SOLDIER IDENTIFICATION
1.
2.
3.
4.
5.Rank
6.Duty MOS/AOC - 75B, 76C, 71L/66H, 70B.
7.Civilian Job Title - Your civilian job occupation with job description.
INCAPACITATION/FITNESS FOR DUTY VERIFICATION
8.INCAPACITATION FOR MILITARY DUTIES.
a.The date of the examination or records review by military physician to determine fitness for duty (year, month, day). Fitness for duty will be determined IAW AR
b.Check appropriate box and complete date* if applicable.
*Length of time indicating fitness for duty cannot exceed 90 days on this form. Subsequent forms must be used for each additional period of incapacitation.
c.Check appropriate box if applicable.
d.Check appropriate box and complete date if applicable.
9.INCAPACITATION FOR CIVILIAN JOB.
a.The date of the examination by any licensed physician to determine fitness for civilian job (year, month, day).
b.Check appropriate box, complete date if applicable.
c.Check appropriate box if applicable.
10.MILITARY PHYSICIAN'S VERIFICATION AND NEXT APPOINTMENT.
a.The attending physician will enter the diagnosis and prognosis.
b.Date of next
c.Name of the military hospital where treatment is received.
d.Name of attending physician.
e.Rank of attending physician, i.e. CPT, LTC, COL.
f.Daytime phone number of physician.
g.Fax Number for attending physician.
h.Signature of attending physician (see note *).
i.
j.The date the form was signed by the attending physician (year, month, day).
*Personnel authorized to sign as a physician are as follows:
(a)Licensed government physician/military physician (Active Army or reserve) assigned to the U.S. Army or other military service.
(b)Reserve commissioned officers that are licensed physicians who are employed by the Department of Veterans Affairs (DVA) as physicians.
(c)
Veterans Affairs (DVA), TRICARE contracted physicians and or
military medical support office (MMSO) contracted physicians).
TRICARE and MMSO do not employ physicians; they have a contract to accept payment from TRICARE.
DA FORM |
Page 2 of 2 |
APD PE v1.01ES