
Once you open the online PDF editor by FormsPal, you're able to complete or change false right here and now. Our development team is continuously endeavoring to enhance the tool and help it become even better for users with its cutting-edge functions. Take your experience to a higher level with continuously developing and exciting options we offer! Here's what you'd want to do to begin:
Step 1: Access the PDF file inside our editor by pressing the "Get Form Button" in the top section of this page.
Step 2: This editor will let you modify your PDF file in many different ways. Modify it by including customized text, adjust existing content, and put in a signature - all within a couple of clicks!
This document will require specific information to be entered, thus be certain to take the time to enter what is asked:
1. Start completing the false with a selection of essential fields. Gather all the important information and be sure not a single thing overlooked!
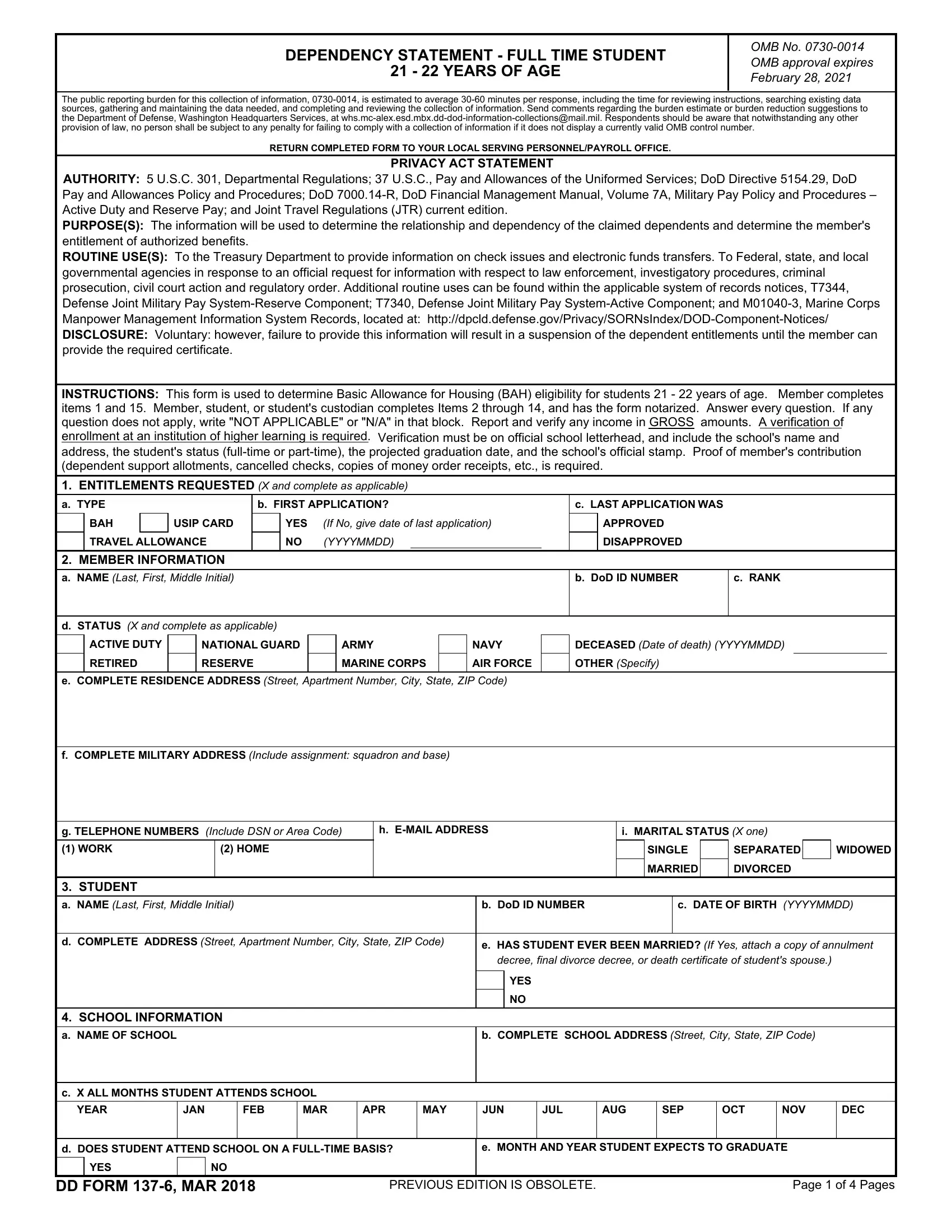
2. Just after performing this section, head on to the subsequent stage and enter all required particulars in these fields - SCHOOL INFORMATION a NAME OF, b COMPLETE SCHOOL ADDRESS Street, c X ALL MONTHS STUDENT ATTENDS, YEAR, JAN, FEB, MAR, APR, MAY, JUN, JUL, AUG, SEP, OCT, and NOV.
People who use this PDF frequently make errors while filling out JUN in this part. Ensure you revise what you enter here.
3. The following step is rather easy, STUDENTS OTHER PARENTS a, NAME Last First Middle Initial, NAME Last First Middle Initial, RELATIONSHIP TO STUDENT, RELATIONSHIP TO STUDENT, COMPLETE ADDRESS Street Apartment, COMPLETE ADDRESS Street Apartment, c ISARE OTHER PARENTS IN ANY, YES, If Yes show rank name SSN and, d DOES OTHER PARENT CLAIM STUDENT, YES, If Yes explain, STUDENTS RESIDENCE a ADDRESS, and b TYPE OF RESIDENCE X and complete - all these empty fields is required to be completed here.
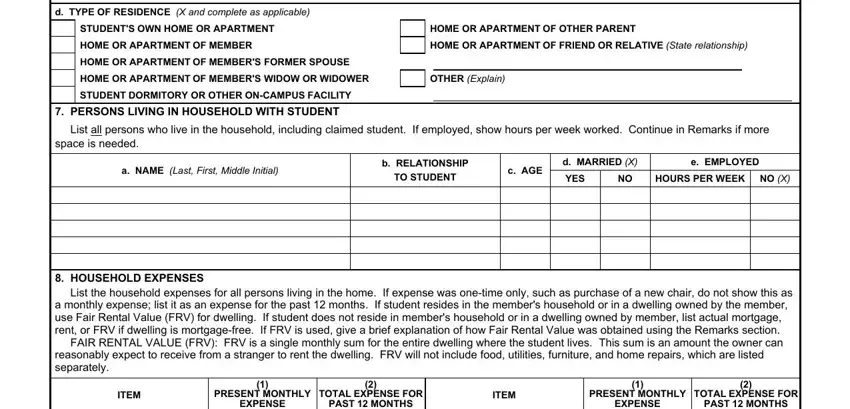
4. This next section requires some additional information. Ensure you complete all the necessary fields - d TYPE OF RESIDENCE X and complete, STUDENTS OWN HOME OR APARTMENT, PERSONS LIVING IN HOUSEHOLD WITH, HOME OR APARTMENT OF OTHER PARENT, OTHER Explain, List all persons who live in the, space is needed, a NAME Last First Middle Initial, b RELATIONSHIP, TO STUDENT, c AGE, d MARRIED X YES NO, e EMPLOYED, HOURS PER WEEK, and NO X - to proceed further in your process!
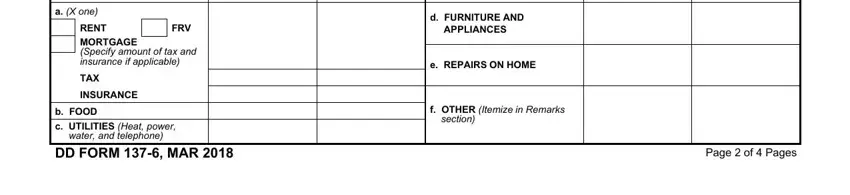
5. The last point to complete this document is pivotal. Make sure to fill out the mandatory fields, such as EXPENSE, a X one, FRV, RENT MORTGAGE Specify amount of, b FOOD c UTILITIES Heat power DD, water and telephone, PAST MONTHS, d FURNITURE AND, APPLIANCES, e REPAIRS ON HOME, f OTHER Itemize in Remarks, section, EXPENSE, PAST MONTHS, and Page of Pages, prior to submitting. Otherwise, it may generate a flawed and potentially invalid paper!
Step 3: Glance through what you have inserted in the blanks and hit the "Done" button. After starting a7-day free trial account at FormsPal, you'll be able to download false or email it at once. The PDF form will also be accessible in your personal account with your each change. FormsPal is focused on the confidentiality of our users; we make sure that all personal information put into our tool stays secure.