
PAYEE can be completed easily. Simply try FormsPal PDF editing tool to perform the job promptly. FormsPal development team is ceaselessly working to enhance the tool and make it much easier for users with its extensive features. Enjoy an ever-improving experience today! If you're seeking to start, here is what it takes:
Step 1: Click the "Get Form" button above. It's going to open up our pdf tool so that you can start filling in your form.
Step 2: The editor lets you change PDF forms in a variety of ways. Change it by including customized text, correct original content, and add a signature - all at your fingertips!
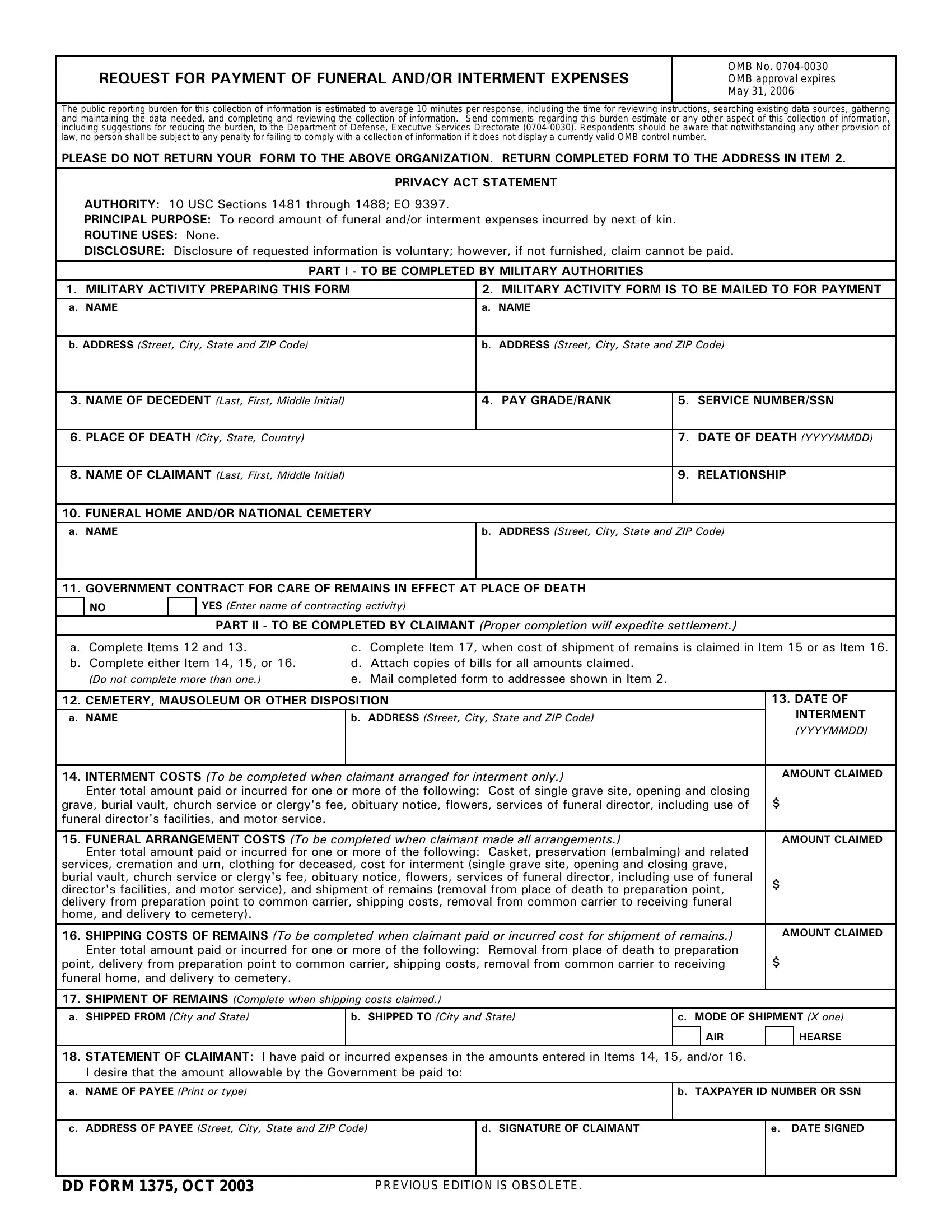
As a way to fill out this PDF form, be sure to enter the information you need in every single blank:
1. It's essential to fill out the PAYEE accurately, so take care while filling out the areas including these fields:
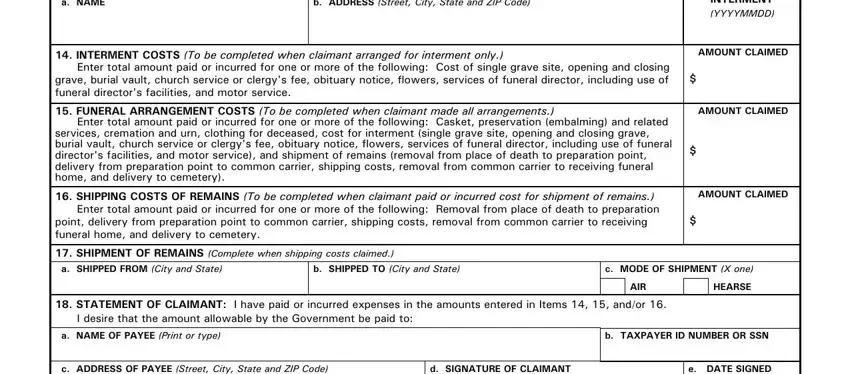
2. The next step is usually to fill in these blanks: CEMETERY MAUSOLEUM OR OTHER, b ADDRESS Street City State and, INTERMENT COSTS To be completed, DATE OF INTERMENT YYYYMMDD, AMOUNT CLAIMED, AMOUNT CLAIMED, SHIPPING COSTS OF REMAINS To be, AMOUNT CLAIMED, SHIPMENT OF REMAINS Complete when, b SHIPPED TO City and State, c MODE OF SHIPMENT X one, AIR, HEARSE, STATEMENT OF CLAIMANT I have paid, and b TAXPAYER ID NUMBER OR SSN.
You can certainly make a mistake while filling in the AIR, thus make sure to look again prior to deciding to send it in.
3. Completing c ADDRESS OF PAYEE Street City, d SIGNATURE OF CLAIMANT, e DATE SIGNED, DD FORM OCT, and PREVIOUS EDITION IS OBSOLETE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: Right after looking through your form fields you've filled in, hit "Done" and you are done and dusted! Download the PAYEE when you subscribe to a 7-day free trial. Conveniently use the pdf form within your personal account page, together with any edits and adjustments being automatically synced! FormsPal is committed to the personal privacy of all our users; we make certain that all personal information processed by our system stays secure.