In today's fast-evolving professional landscape, continuous learning and development play a crucial role in enhancing organizational effectiveness and employee performance. The DD Form 1556 serves as a comprehensive documentation tool for federal employees or military personnel seeking career development through training initiatives. Its multifaceted purpose ranges from requesting training opportunities to authorizing the expenses involved. Specifically designed to cater to the diverse needs of Department of Defense personnel, the form meticulously records various aspects such as the authorization of training expenses, agreements for service continuation post-training, certification of completed training, and any reimbursement clauses tied to the training program. The form mandates disclosures under the Privacy Act, guided by specific U.S. Code sections and executive orders, ensuring transparency and informed consent from the participants. Additionally, it plays a pivotal role in managing and recording the intricate financial transactions associated with training programs, which can vary from tuition fees to travel expenses, thereby serving both administrative efficiency and regulatory compliance within the Department of Defense's robust training ecosystem.
| Question | Answer |
|---|---|
| Form Name | Dd Form 1556 |
| Form Length | 13 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 15 sec |
| Other names | dd form 1556, form 1556 1, DSN, 1st |
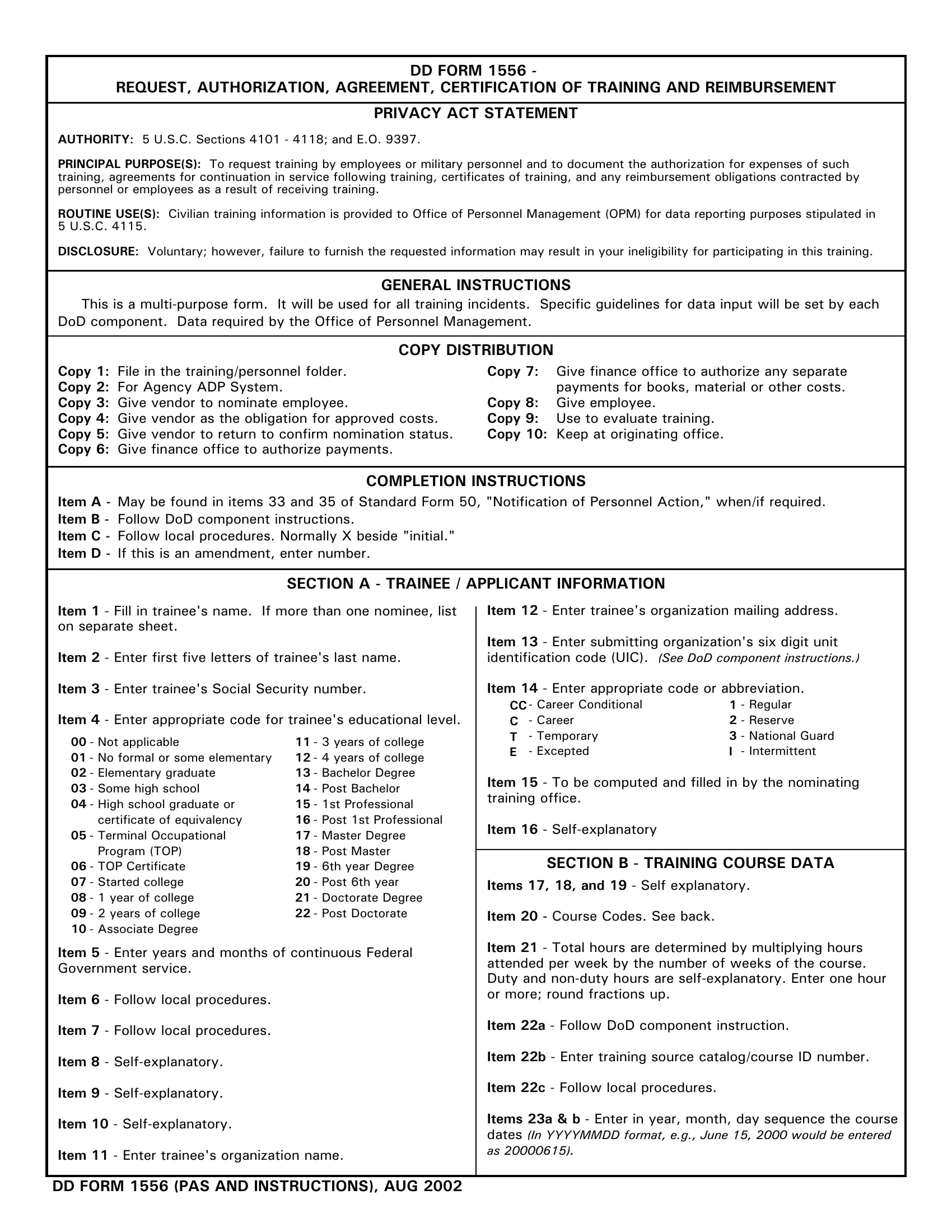
DD FORM 1556 -
REQUEST, AUTHORIZATION, AGREEMENT, CERTIFICATION OF TRAINING AND REIMBURSEMENT
PRIVACY ACT STATEMENT
AUTHORITY: 5 U.S.C. Sections 4101 - 4118; and E.O. 9397.
PRINCIPAL PURPOSE(S): To request training by employees or military personnel and to document the authorization for expenses of such training, agreements for continuation in service following training, certificates of training, and any reimbursement obligations contracted by personnel or employees as a result of receiving training.
ROUTINE USE(S): Civilian training information is provided to Office of Personnel Management (OPM) for data reporting purposes stipulated in 5 U.S.C. 4115.
DISCLOSURE: Voluntary; however, failure to furnish the requested information may result in your ineligibility for participating in this training.
GENERAL INSTRUCTIONS
This is a
COPY DISTRIBUTION
Copy 1: File in the training/personnel folder. |
Copy 7: |
Give finance office to authorize any separate |
Copy 2: For Agency ADP System. |
|
payments for books, material or other costs. |
Copy 3: Give vendor to nominate employee. |
Copy 8: |
Give employee. |
Copy 4: Give vendor as the obligation for approved costs. |
Copy 9: |
Use to evaluate training. |
Copy 5: Give vendor to return to confirm nomination status. |
Copy 10: Keep at originating office. |
|
Copy 6: Give finance office to authorize payments. |
|
|
COMPLETION INSTRUCTIONS
Item A - May be found in items 33 and 35 of Standard Form 50, "Notification of Personnel Action," when/if required. Item B - Follow DoD component instructions.
Item C - Follow local procedures. Normally X beside "initial." Item D - If this is an amendment, enter number.
SECTION A - TRAINEE / APPLICANT INFORMATION
Item 1 - Fill in trainee's name. If more than one nominee, list |
Item 12 - Enter trainee's organization mailing address. |
|||||||
on separate sheet. |
|
|
Item 13 - Enter submitting organization's six digit unit |
|||||
|
|
|
|
|||||
Item 2 - Enter first five letters of trainee's last name. |
identification code (UIC). (See DoD component instructions.) |
|||||||
Item 3 - Enter trainee's Social Security number. |
Item 14 - Enter appropriate code or abbreviation. |
|||||||
Item 4 - Enter appropriate code for trainee's educational level. |
CC - Career Conditional |
1 - Regular |
||||||
C |
- Career |
2 - Reserve |
||||||
00 |
- Not applicable |
11 |
- 3 years of college |
T |
- Temporary |
3 - National Guard |
||
E |
- Excepted |
I - Intermittent |
||||||
01 |
- No formal or some elementary |
12 |
- 4 years of college |
|||||
|
|
|
|
|||||
02 |
- Elementary graduate |
13 |
- Bachelor Degree |
Item 15 - To be computed and filled in by the nominating |
||||
03 |
- Some high school |
14 |
- Post Bachelor |
|||||
training office. |
|
|
||||||
04 |
- High school graduate or |
15 |
- 1st Professional |
|
|
|||
|
|
|
|
|||||
|
certificate of equivalency |
16 |
- Post 1st Professional |
Item 16 - |
|
|
||
05 |
- Terminal Occupational |
17 |
- Master Degree |
|
|
|||
|
|
|
|
|||||
|
Program (TOP) |
18 |
- Post Master |
|
|
|
|
|
|
|
SECTION B - TRAINING COURSE DATA |
|
|||||
06 |
- TOP Certificate |
19 |
- 6th year Degree |
|
|
|||
07 |
- Started college |
20 |
- Post 6th year |
Items 17, 18, and 19 - Self explanatory. |
|
|||
08 |
- 1 year of college |
21 |
- Doctorate Degree |
|
|
|
|
|
09 |
- 2 years of college |
22 |
- Post Doctorate |
Item 20 - Course Codes. See back. |
|
|
||
10 |
- Associate Degree |
|
|
|
|
|
|
|
Item 5 - Enter years and months of continuous Federal |
Item 21 - Total hours are determined by multiplying hours |
|||||||
attended per week by the number of weeks of the course. |
||||||||
Government service. |
|
|
||||||
|
|
Duty and |
||||||
|
|
|
|
|||||
Item 6 - Follow local procedures. |
|
|
or more; round fractions up. |
|
|
|||
|
|
|
|
|
|
|||
Item 7 - Follow local procedures. |
|
|
Item 22a - Follow DoD component instruction. |
|||||
|
|
|
|
|
|
|||
Item 8 - |
|
|
Item 22b - Enter training source catalog/course ID number. |
|||||
|
|
|
|
|
|
|||
Item 9 - |
|
|
Item 22c - Follow local procedures. |
|
|
|||
|
|
|
|
|
|
|||
Item 10 - |
|
|
Items 23a & b - Enter in year, month, day sequence the course |
|||||
|
|
dates (In YYYYMMDD format, e.g., June 15, 2000 would be entered |
||||||
|
|
|
|
|||||
Item 11 - Enter trainee's organization name. |
as 20000615). |
|
|
|||||
|
|
|
|
|||||
DD FORM 1556 (PAS AND INSTRUCTIONS), AUG 2002
DD FORM 1556 INSTRUCTIONS (Continued)
|
|
|
SECTION B - TRAINING COURSE DATA (Continued) |
|
SECTION C - COSTS AND BILLING INFORMATION |
|
|
||||
|
|
Item 20 - COURSE CODES - Enter appropriate codes from |
|
Item 24 - X if applicable. |
|
|
|||||
|
|
|
|||||||||
|
|
those listed below. |
|
|
|
|
Items 25a & b - Enter dollars and cents. |
||||
|
|
|
|
|
|
|
|
|
|||
|
|
A - PURPOSE |
|
|
|
|
|
Item 25c - Sum of items 25a & b. (See Note below) |
|||
1 |
- Mission or program change |
5 - Meet future staffing needs |
|
Item 25d - Follow DoD component instructions. |
|||||||
2 |
- New technology |
|
6 - Develop unavailable skills |
|
|||||||
|
|
|
|
|
|||||||
3 |
- New work assignment |
7 - Trade or craft apprenticeship |
|
Items 26a & b - Enter dollars and cents. |
|||||||
4 |
- Improve present |
|
8 - Orientation |
|
|
|
|
||||
|
|
|
performance |
|
9 - Adult basic education |
|
Item 26c - Sum of items 26a & b. (See Note below) |
||||
|
|
B - TYPE |
|
|
|
|
|
Items 27 & 29 - For finance office use. Enter only one |
|||
1 |
- Executive and management |
5 - Specialty and technical |
|
accounting classification on each DD 1556. |
|||||||
|
|
|
|
||||||||
2 |
- Supervisory |
|
|
6 - Clerical |
|
Items 28 & 31 - Follow local procedures. |
|||||
3 |
- Legal, medical, scientific or |
7 - Trade or craft |
|
||||||||
|
|
|
|
||||||||
|
|
|
engineering |
|
|
8 - Orientation |
|
Item 30 - Sum of items 25c & 26c. |
|||
4 |
- Administration and analysis |
9 - Adult basic education |
|
Note: For a group, totals are for all trainees. |
|||||||
|
|
C - SOURCE |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||
|
|
A - US Army |
|
S - Defense Logistics Agency |
|
SECTION D - APPROVALS/CONCURRENCE/ |
|
|
|||
|
|
D - Other DoD |
|
2 - |
|
CERTIFICATION |
|
|
|||
|
|
F - US Air Force |
|
3 - |
|
|
|
|
|||
|
|
Item 32 - To be certified/signed by supervisor of trainee. |
|||||||||
|
|
M - US Marine Corps |
4 - |
|
|||||||
|
|
|
|
|
|
||||||
|
|
N - US Navy |
|
5 - State or local Government |
|
Item 33 - To be certified/signed by the official designated CPO |
|||||
|
|
|
|
|
|
|
|
|
|||
|
|
D - SPECIAL INTEREST |
|
|
|
Head of Training. |
|||||
|
|
|
|
|
|
|
|
||||
|
|
0 - No special program |
1 - Executive Development 2 - Supervision |
|
Item 34 - Follow local procedures. |
||||||
|
|
E - TRAINING VENDOR |
|
|
|
Item 35 - School official complete, sign, date and return |
|||||
|
|
|
Follow DoD component instructions. |
|
copy 5. |
||||||
|
|
F - SECURITY CLEARANCE OF COURSE |
|
Item 36 - If course completed, enter date and grade; if not, |
|||||||
|
|
U - Unclassified |
C - Confidential |
S - Secret T - Top Secret |
|
return form with explanatory memo to Training Officer |
|||||
|
|
|
identified in item 33. |
||||||||
|
|
|
|
|
|
|
|
|
|||
|
|
G - ALLOCATION STATUS |
|
|
|
Items 37 & 38 - Follow local procedures. |
|||||
|
|
1- Primary 2 - Alternate |
3 - Space Available |
|
|||||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H - PRIORITY |
|
|
|
|
|
SECTION E - TRAINEE AGREEMENT/CERTIFICATION |
|
|
|
|
|
|
|
|
|
|
(Back of Copy 1) |
|
|
||
|
|
|
Enter priority 1, 2, or 3 in accordance with DoD Instruction |
|
|
|
|||||
|
|
|
|
The trainee (applicant) must read and understand the |
|
|
|||||
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
statements contained in this section. If there are any |
||
|
|
I - TRAINING LEVEL |
|
|
|
|
questions, please contact the nominating activity Training |
||||
1 |
- Elementary |
3 - Vocational/ |
|
4 - College, undergraduate |
|
Office. |
|||||
|
|
|
|
|
|||||||
2 |
- High School |
Technical/Secretarial/ |
5 - College, graduate |
|
Item 38f - To be completed by nominating Training Office. |
||||||
|
|
|
|
Business/Commercial/ 6 - College, post graduate |
|
||||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
Administrative |
|
|
|
Item 39 - To be signed and dated by employee nominated for |
|||
|
|
|
|
|
|
|
|
|
|||
|
|
J - METHOD OF TRAINING |
|
|
|
||||||
|
|
|
|
|
|
|
|
||||
1 |
- |
|
6 - Directed study |
|
SECTION F - TRAINING VENDOR |
|
|
||||
2 |
- Rotation of work assignment |
|
7 - Classroom (resident) |
|
(Back of Copies 3, 4 & 5) |
|
|
||||
3 |
- Seminar (training) |
|
|
8 - Classroom (on site) |
|
|
|
|
|||
|
|
|
Items 40 & 43 - Instructions on back of copy 3. |
||||||||
4 |
- Conference/meeting/symposium |
9 - Test/Equivalency |
|
||||||||
|
|
|
|
||||||||
5 |
- Correspondence |
|
|
|
|
Item 44 - Back of Copy 5 - Mailing Address Nominating |
|||||
|
|
|
|
|
|
|
|
|
|||
|
|
K - TRAINING PROGRAM |
|
|
|
Agency - To be filled in by nominating Training Office. |
|||||
|
|
|
|
|
|
|
|
||||
|
|
|
Follow DoD component instructions. |
|
|
|
|
||||
|
|
|
|
SECTION G - FINANCE |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L - REASON FOR SELECTION OF COURSE |
|
(Back of Copies 6 & 7) |
|
|
|||||
1 |
- Quality of training |
|
|
|
|
Items 45, 46, or 47 as appropriate, filled in by the nominating |
|
|
|||
|
|
|
|
|
|||||||
2 |
- Most cost effective |
|
|
|
|
activity Training Office. |
|||||
3 |
- Unique capability of training source |
|
|
|
|
|
|||||
|
|
SECTION H - EVALUATION |
|
|
|||||||
4 |
- Location |
|
|
|
|
|
|
|
|||
5 |
- Not available in Government |
|
|
|
(Copy 9) |
|
|
||||
6 |
- Incidental to procurement of equipment |
|
|
To be completed by trainee and immediate supervisor after |
|
|
|||||
|
|
|
|||||||||
7 |
- Timeliness |
|
|
|
|
|
training is completed (following agency instructions). |
||||
DD FORM 1556 (PAS AND INSTRUCTIONS) (BACK), AUG 2002