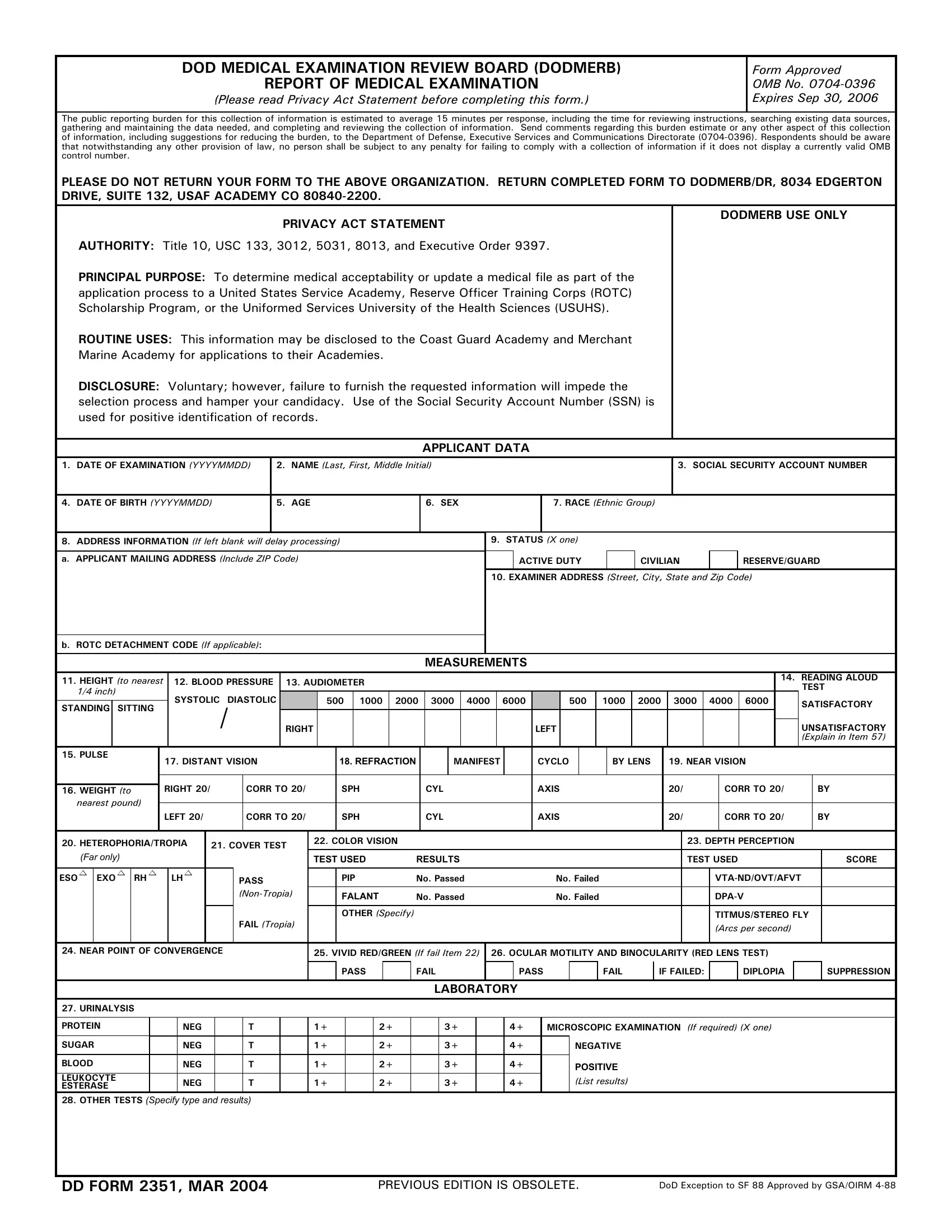
Embarking on the journey to serve in a United States Service Academy, Reserve Officer Training Corps (ROTC) Scholarship Program, or the Uniformed Services University of the Health Sciences requires completion of various prerequisites, one of which includes the essential DD 2351 form. Known as the DOD Medical Examination Review Board (DODMERB) Report of Medical Examination, this document serves as a critical step in determining applicants' medical eligibility to join the esteemed ranks of the military. With a collection of items designed to evaluate an applicant's physical and mental health, the form is meticulously structured to cover an exhaustive array of medical aspects from visual and auditory acuity to cardiovascular health and beyond. As outlined by the Privacy Act Statement, the form not only seeks to confirm the medical readiness of future military personnel but also ensures the privacy and protection of applicants’ personal information, making its completion a task of both significance and sensitivity. With the approach of its expiration on September 30, 2006, individuals are reminded of the importance of carefully reading the instructions and accurately completing the form to facilitate a smooth application process. The DD 2351 form, therefore, stands not just as a mere procedural requirement but as a fundamental gateway to furthering one's commitment to serving their country.
| Question | Answer |
|---|---|
| Form Name | Dd Form 2351 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | medical exam form pdf, doctors exam form, pcv medical form, physical exam form |
DOD MEDICAL EXAMINATION REVIEW BOARD (DODMERB) |
Form Approved |
REPORT OF MEDICAL EXAMINATION |
OMB No. |
(Please read Privacy Act Statement before completing this form.) |
Expires Sep 30, 2006 |
The public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to the Department of Defense, Executive Services and Communications Directorate
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION. RETURN COMPLETED FORM TO DODMERB/DR, 8034 EDGERTON DRIVE, SUITE 132, USAF ACADEMY CO
PRIVACY ACT STATEMENT
AUTHORITY: Title 10, USC 133, 3012, 5031, 8013, and Executive Order 9397.
PRINCIPAL PURPOSE: To determine medical acceptability or update a medical file as part of the application process to a United States Service Academy, Reserve Officer Training Corps (ROTC) Scholarship Program, or the Uniformed Services University of the Health Sciences (USUHS).
ROUTINE USES: This information may be disclosed to the Coast Guard Academy and Merchant Marine Academy for applications to their Academies.
DISCLOSURE: Voluntary; however, failure to furnish the requested information will impede the selection process and hamper your candidacy. Use of the Social Security Account Number (SSN) is used for positive identification of records.
DODMERB USE ONLY
APPLICANT DATA
1. DATE OF EXAMINATION (YYYYMMDD)
2.NAME (Last, First, Middle Initial)
3. SOCIAL SECURITY ACCOUNT NUMBER
4. DATE OF BIRTH (YYYYMMDD)
5. AGE
6. SEX
7.RACE (Ethnic Group)
8.ADDRESS INFORMATION (If left blank will delay processing) A. APPLICANT MAILING ADDRESS (Include ZIP Code)
9. STATUS (X one)
|
ACTIVE DUTY |
|
CIVILIAN |
|
RESERVE/GUARD |
|
|
|
|
|
|
10.EXAMINER ADDRESS (Street, City, State and Zip Code)
B. ROTC DETACHMENT CODE (If applicable):
MEASUREMENTS
11. HEIGHT (to nearest |
|
12. BLOOD PRESSURE |
13. AUDIOMETER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. READING ALOUD |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST |
||||||||||||||||||||||||||||
1/4 inch) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
SYSTOLIC DIASTOLIC |
|
|
500 |
1000 |
|
2000 |
|
3000 |
4000 |
|
6000 |
|
500 |
|
1000 |
2000 |
3000 |
|
4000 |
6000 |
|
|
|
SATISFACTORY |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
STANDING |
|
SITTING |
|
|
|
|
|
/ |
|
|
RIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEFT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNSATISFACTORY |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Explain in Item 57) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. PULSE |
|
|
|
|
|
|
17. DISTANT VISION |
|
18. REFRACTION |
|
|
|
MANIFEST |
|
|
|
CYCLO |
|
|
|
BY LENS |
|
19. NEAR VISION |
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
RIGHT 20/ |
|
|
CORR TO 20/ |
|
SPH |
|
|
CYL |
|
|
|
AXIS |
|
|
|
|
20/ |
|
|
CORR TO 20/ |
|
BY |
|||||||||||||||||||||||||
16. WEIGHT (to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
nearest pound) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
LEFT 20/ |
|
|
CORR TO 20/ |
|
SPH |
|
|
CYL |
|
|
|
AXIS |
|
|
|
|
20/ |
|
|
CORR TO 20/ |
|
BY |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
20. HETEROPHORIA/TROPIA |
|
21. COVER TEST |
|
22. COLOR VISION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. DEPTH PERCEPTION |
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
(Far only) |
|
|
|
|
|
|
|
|
|
|
TEST USED |
RESULTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TEST USED |
|
|
SCORE |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
ESO |
|
|
EXO |
|
|
RH |
|
|
|
LH |
|
|
|
|
PASS |
|
|
PIP |
NO. PASSED |
|
|
|
NO. FAILED |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FALANT |
NO. PASSED |
|
|
|
NO. FAILED |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FAIL (Tropia) |
|
|
OTHER (Specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TITMUS/STEREO FLY |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Arcs per second) |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
24. NEAR POINT OF CONVERGENCE |
|
|
|
|
25. VIVID RED/GREEN (If fail Item 22) |
26. OCULAR MOTILITY AND BINOCULARITY (RED LENS TEST) |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASS |
|
|
FAIL |
|
|
|
PASS |
|
|
FAIL |
|
IF FAILED: |
|
|
DIPLOPIA |
|
|
|
SUPPRESSION |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
27.URINALYSIS PROTEIN SUGAR
BLOOD
LEUKOCYTE
ESTERASE
|
NEG |
|
T |
|
1+ |
|
2+ |
|
3+ |
|
4+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
NEG |
|
T |
|
1+ |
|
2+ |
|
3+ |
|
4+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
NEG |
|
T |
|
1+ |
|
2+ |
|
3+ |
|
4+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
NEG |
|
T |
|
1+ |
|
2+ |
|
3+ |
|
4+ |
|
|
|
|
|
|
|
|
|
|
|
|
MICROSCOPIC EXAMINATION (If required) (X one)
NEGATIVE
POSITIVE
(List results)
28.OTHER TESTS (Specify type and results)
DD FORM 2351, MAR 2004 |
PREVIOUS EDITION IS OBSOLETE. |
DoD Exception to SF 88 Approved by GSA/OIRM |
CLINICAL EVALUATION
NORMAL |
|
(X each item in the appropriate column. |
ABNOR- |
NORMAL |
|
|
(X each item in the appropriate column. |
ABNOR- |
||
|
Enter "NE" if not evaluated) |
|
MAL |
|
|
Enter "NE" if not evaluated) |
MAL |
|||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
29. |
HEAD, FACE, NECK AND SCALP |
|
|
|
43. |
ABDOMEN AND VISCERA (Include hernia) |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
30. |
NOSE |
|
|
|
44. |
ENDOCRINE SYSTEM |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
31. |
SINUSES |
|
|
|
45. |
SPINE, OTHER MUSCULOSKELETAL |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
32. |
MOUTH AND THROAT |
|
|
|
46. |
UPPER EXTREMITIES (Strength, sensation, |
|
||
|
33. |
EARS - GENERAL(Internal and external canals) |
|
|
|
range of motion) |
|
|||
|
|
|
|
|
|
|
|
|||
|
|
(Auditory acuity under item 13) |
|
|
|
47. |
LOWER EXTREMITIES (Except feet) (Strength, |
|
||
|
|
|
|
|
|
|
||||
|
34. |
DRUMS (Perforation) |
|
|
|
|
sensation, range of motion) |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
35. |
VALSALVA |
|
|
|
48. |
FEET |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
36. |
EYES - GENERAL (Visual acuity and refraction |
|
|
49. |
IDENTIFYING BODY MARKS, SCARS, TATTOOS |
|
|||
|
|
under items 17, 18, and 19) |
|
|
|
50. |
SKIN, LYMPHATICS |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
37. |
PUPILS (Equality and reaction) |
|
|
|
51. |
GU SYSTEM |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
38. |
OCULAR MOTILITY (Associated parallel |
|
|
|
52. |
ANUS AND RECTUM (Hemorrhoids, fistulae) |
|
||
|
|
movements, nystagmus) |
|
|
|
|
(Prostate if indicated) EXTERNAL EXAM |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
39. |
OPHTHALMOSCOPIC |
|
|
|
53. |
FEMALE GU EXTERNAL VISUAL EXAM |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
40. |
LUNGS AND CHEST (Include breasts) |
|
|
|
54. |
NEUROLOGIC |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
41. |
HEART (Thrust, size, rhythm, and sounds) |
|
|
55. |
PSYCHIATRIC (Specify any personality deviation) |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
42. |
VASCULAR SYSTEM (Varicosities, etc.) |
|
|
|
|
|
|
|
|
56. REPEAT BP OR PULSE EXAM (SITTING) IF BP >140/90 OR PULSE >100 |
|
|
|
|
|
|
||||
|
|
|
|
|||||||
57. NOTES (Describe every abnormality in detail. Enter the item number before each comment.) |
|
|||||||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
58. EXAMINER (If performed by PA, PCNP, OR FNP) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||||
TYPED OR PRINTED NAME |
RANK |
|
CORPS OR DEGREE |
|
SIGNATURE |
|
||||
|
|
|
|
|
|
|
|
|
||
59. PHYSICIAN (MD/DO) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||
TYPED OR PRINTED NAME |
RANK |
|
DEGREE |
|
|
SIGNATURE |
|
|||
DD FORM 2351 (BACK), MAR 2004