

With the online editor for PDFs by FormsPal, you may complete or edit OMB right here and now. The editor is continually improved by our team, receiving cool functions and turning out to be much more convenient. This is what you would need to do to start:
Step 1: Click on the "Get Form" button above on this webpage to get into our PDF editor.
Step 2: Once you start the file editor, you will get the document prepared to be filled in. Other than filling out various fields, you may as well do several other actions with the Document, particularly putting on any text, modifying the initial textual content, adding illustrations or photos, putting your signature on the document, and more.
When it comes to blank fields of this precise PDF, here's what you should do:
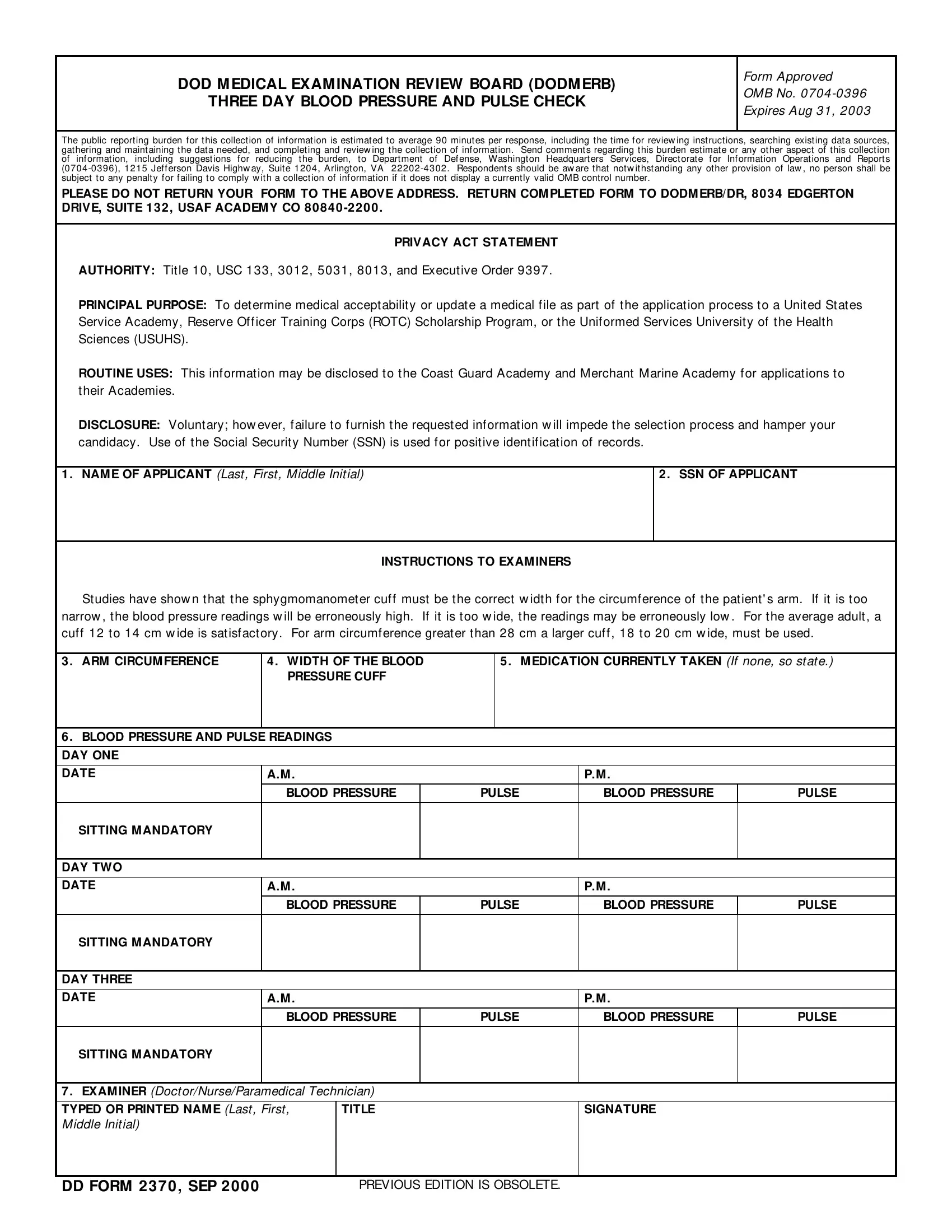
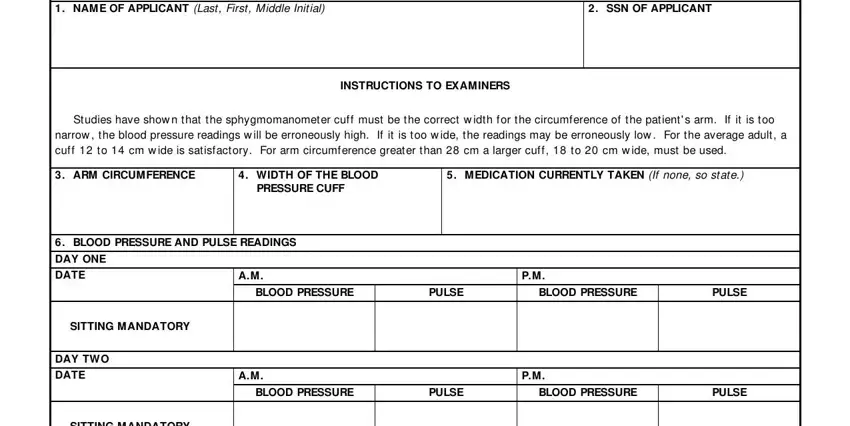
1. When filling in the OMB, make certain to include all important blanks in its relevant part. It will help facilitate the work, which allows your details to be processed without delay and properly.
2. Right after performing the previous step, go on to the next part and fill out all required particulars in these blank fields - DAY THREE, DATE, SITTING MANDATORY, BLOOD PRESSURE, PULSE, BLOOD PRESSURE, PULSE, EXAMINER DoctorNurseParamedical, SIGNATURE, DD FORM SEP, and PREVIOUS EDITION IS OBSOLETE.
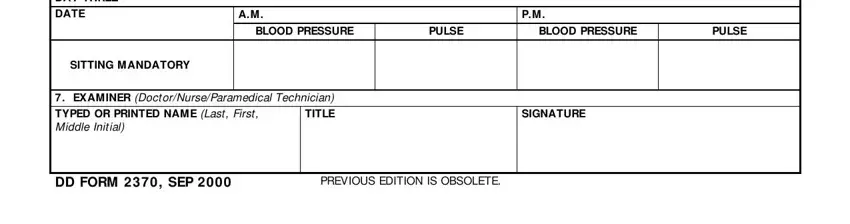
People generally make errors when completing PULSE in this area. Don't forget to double-check everything you enter here.
Step 3: Prior to submitting your file, ensure that all blanks have been filled out the right way. When you think it is all good, click on “Done." Make a free trial account with us and get direct access to OMB - with all changes preserved and available in your FormsPal cabinet. When you work with FormsPal, you can fill out documents without the need to worry about database incidents or entries being distributed. Our protected system ensures that your personal details are maintained safely.