|
|
|
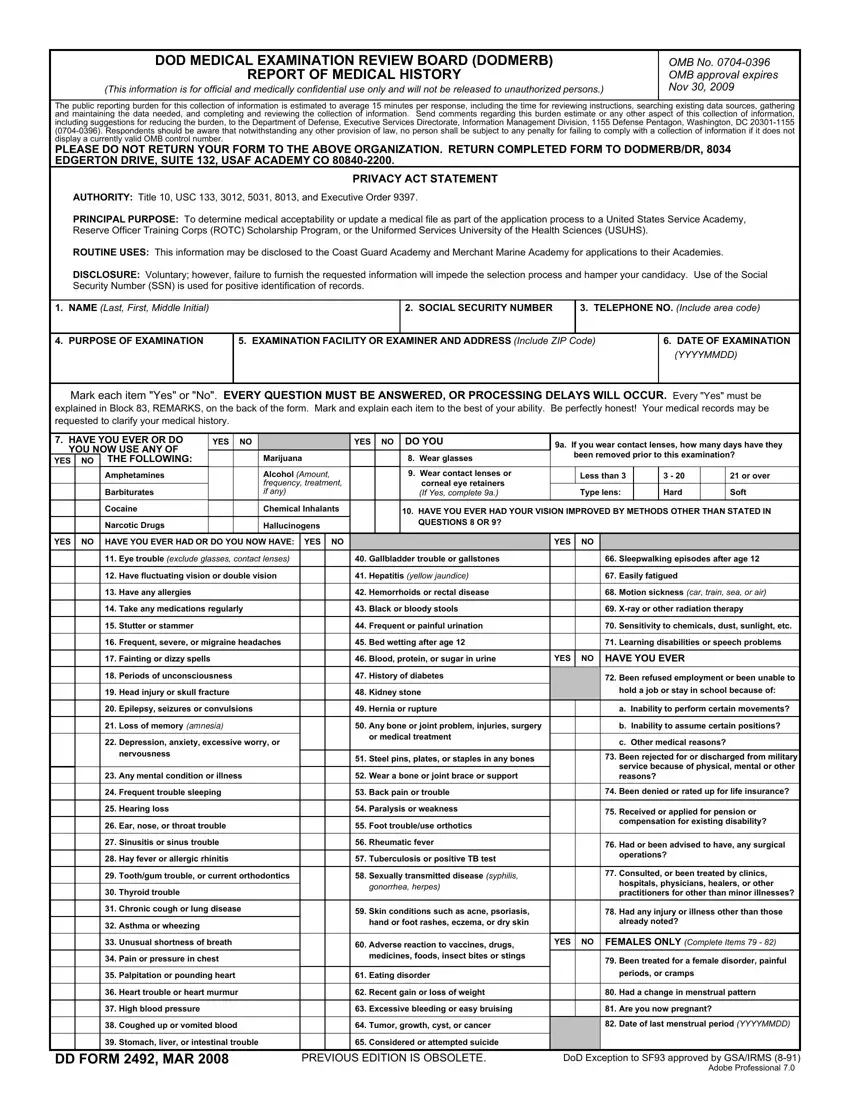
DOD MEDICAL EXAMINATION REVIEW BOARD (DODMERB) |
|
|
|
|
OMB No. 0704-0396 |
|
|
|
|
|
|
|
REPORT OF MEDICAL HISTORY |
|
|
|
|
OMB approval expires |
|
|
(This information is for official and medically confidential use only and will not be released to unauthorized persons.) |
NOV 30, 2009 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering |
and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, |
including suggestions for reducing the burden, to the Department of Defense, Executive Services Directorate, Information Management Division, 1155 Defense Pentagon, Washington, DC 20301-1155 |
(0704-0396). Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to any penalty for failing to comply with a collection of information if it does not |
display a currently valid OMB control number. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION. RETURN COMPLETED FORM TO DODMERB/DR, 8034 |
EDGERTON DRIVE, SUITE 132, USAF ACADEMY CO 80840-2200. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIVACY ACT STATEMENT |
|
|
|
|
|
|
|
|
|
AUTHORITY: Title 10, USC 133, 3012, 5031, 8013, and Executive Order 9397. |
|
|
|
|
|
|
|
|
|
PRINCIPAL PURPOSE: To determine medical acceptability or update a medical file as part of the application process to a United States Service Academy, |
|
Reserve Officer Training Corps (ROTC) Scholarship Program, or the Uniformed Services University of the Health Sciences (USUHS). |
|
|
|
|
|
ROUTINE USES: This information may be disclosed to the Coast Guard Academy and Merchant Marine Academy for applications to their Academies. |
|
|
DISCLOSURE: Voluntary; however, failure to furnish the requested information will impede the selection process and hamper your candidacy. Use of the Social |
|
Security Number (SSN) is used for positive identification of records. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
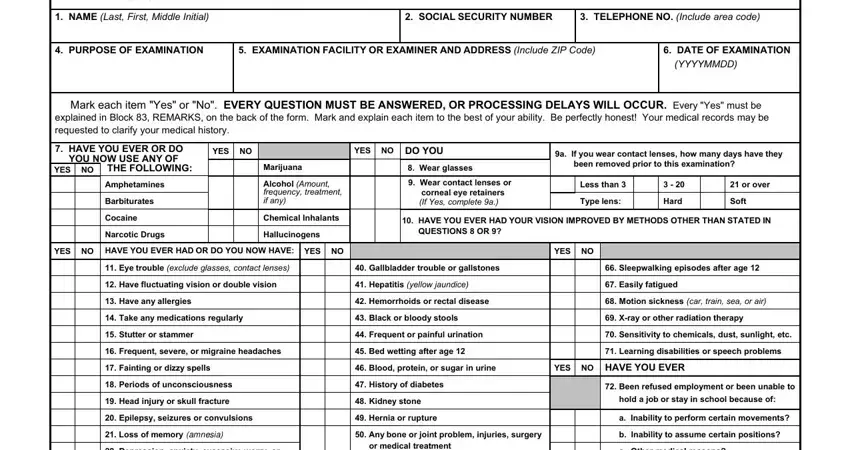
1. NAME (Last, First, Middle Initial) |
|
|
|
|
|
|
|
|
|
2. SOCIAL SECURITY NUMBER |
|
3. TELEPHONE NO. (Include area code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. PURPOSE OF EXAMINATION |
|
|
5. EXAMINATION FACILITY OR EXAMINER AND ADDRESS (Include ZIP Code) |
6. DATE OF EXAMINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mark each item "Yes" or "No". EVERY QUESTION MUST BE ANSWERED, OR PROCESSING DELAYS WILL OCCUR. Every "Yes" must be |
explained in Block 83, REMARKS, on the back of the form. Mark and explain each item to the best of your ability. Be perfectly honest! Your medical records may be |
requested to clarify your medical history. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. HAVE YOU EVER OR DO |
|
YES |
|
NO |
|
|
|
YES |
NO |
DO YOU |
9a. If you wear contact lenses, how many days have they |
YOU NOW USE ANY OF |
|
|
|
|
Marijuana |
|
|
|
8. Wear glasses |
|
been removed prior to this examination? |
YES |
NO |
THE FOLLOWING: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amphetamines |
|
|
|
|
Alcohol (Amount, |
|
|
|
9. Wear contact lenses or |
|
Less than 3 |
|
3 - 20 |
|
|
21 or over |
|
|
|
|
|
|
|
|
frequency, treatment, |
|
|
|
corneal eye retainers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Barbiturates |
|
|
|
|
if any) |
|
|
|
(If Yes, complete 9a.) |
|
Type lens: |
|
Hard |
|
|
Soft |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cocaine |
|
|
|
|
Chemical Inhalants |
|
|
|
10. HAVE YOU EVER HAD YOUR VISION IMPROVED BY METHODS OTHER THAN STATED IN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narcotic Drugs |
|
|
|
|
Hallucinogens |
|
|
|
QUESTIONS 8 OR 9? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
HAVE YOU EVER HAD OR DO YOU NOW HAVE: |
YES |
NO |
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
11. |
Eye trouble (exclude glasses, contact lenses) |
|
|
40. |
Gallbladder trouble or gallstones |
|
|
66. Sleepwalking episodes after age 12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. |
Have fluctuating vision or double vision |
|
|
41. |
Hepatitis (yellow jaundice) |
|
|
67. Easily fatigued |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. |
Have any allergies |
|
|
|
|
|
|
42. |
Hemorrhoids or rectal disease |
|
|
68. Motion sickness (car, train, sea, or air) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. |
Take any medications regularly |
|
|
43. |
Black or bloody stools |
|
|
69. X-ray or other radiation therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
Stutter or stammer |
|
|
|
|
|
|
44. |
Frequent or painful urination |
|
|
70. Sensitivity to chemicals, dust, sunlight, etc. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. |
Frequent, severe, or migraine headaches |
|
|
45. |
Bed wetting after age 12 |
|
|
71. Learning disabilities or speech problems |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. |
Fainting or dizzy spells |
|
|
|
|
|
|
46. |
Blood, protein, or sugar in urine |
YES |
NO |
HAVE YOU EVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. |
Periods of unconsciousness |
|
|
|
|
47. |
History of diabetes |
|
|
72. Been refused employment or been unable to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. |
Head injury or skull fracture |
|
|
|
|
48. |
Kidney stone |
|
|
hold a job or stay in school because of: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. |
Epilepsy, seizures or convulsions |
|
|
49. |
Hernia or rupture |
|
|
a. Inability to perform certain movements? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. |
Loss of memory (AMNESIA) |
|
|
|
|
50. |
Any bone or joint problem, injuries, surgery |
|
|
b. Inability to assume certain positions? |
|
|
|
|
|
|
|
|
|
|
|
|
or medical treatment |
|
|
|
|
|
|
|
|
|
|
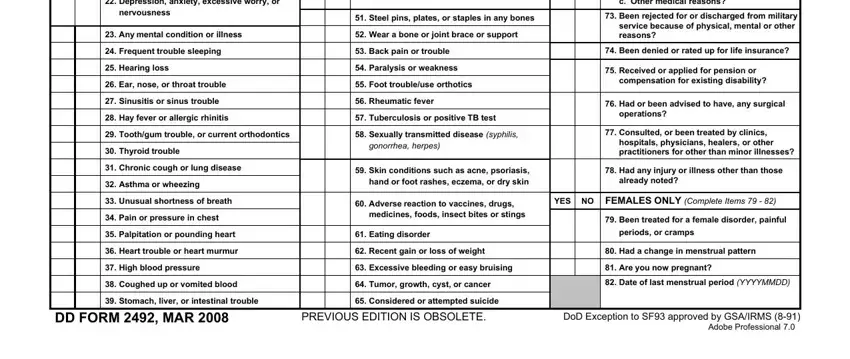
22. |
Depression, anxiety, excessive worry, or |
|
|
|
|
|
c. Other medical reasons? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
nervousness |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
51. |
Steel pins, plates, or staples in any bones |
|
|
73. Been rejected for or discharged from military |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
service because of physical, mental or other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. |
Any mental condition or illness |
|
|
52. |
Wear a bone or joint brace or support |
|
|
|
|
|
|
|
|
reasons? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. |
Frequent trouble sleeping |
|
|
|
|
53. |
Back pain or trouble |
|
|
74. Been denied or rated up for life insurance? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. |
Hearing loss |
|
|
|
|
|
|
54. |
Paralysis or weakness |
|
|
75. Received or applied for pension or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26. |
Ear, nose, or throat trouble |
|
|
|
|
55. |
Foot trouble/use orthotics |
|
|
compensation for existing disability? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27. |
Sinusitis or sinus trouble |
|
|
|
|
56. |
Rheumatic fever |
|
|
76. Had or been advised to have, any surgical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. |
Hay fever or allergic rhinitis |
|
|
|
|
57. |
Tuberculosis or positive TB test |
|
|
operations? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29. |
Tooth/gum trouble, or current orthodontics |
|
|
58. |
Sexually transmitted disease (syphilis, |
|
|
77. Consulted, or been treated by clinics, |
|
|
|
|
|
|
hospitals, physicians, healers, or other |
|
|
|
|
|
|
|
|
|
|
|
|
gonorrhea, herpes) |
|
|
|
|
30. |
Thyroid trouble |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
practitioners for other than minor illnesses? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31. |
Chronic cough or lung disease |
|
|
59. |
Skin conditions such as acne, psoriasis, |
|
|
78. Had any injury or illness other than those |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32. |
Asthma or wheezing |
|
|
|
|
|
|
|
hand or foot rashes, eczema, or dry skin |
|
|
already noted? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
33. |
Unusual shortness of breath |
|
|
|
|
60. |
Adverse reaction to vaccines, drugs, |
YES |
NO |
FEMALES ONLY (Complete Items 79 - 82) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. |
Pain or pressure in chest |
|
|
|
|
|
medicines, foods, insect bites or stings |
|
|
79. Been treated for a female disorder, painful |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
35. |
Palpitation or pounding heart |
|
|
|
|
61. |
Eating disorder |
|
|
periods, or cramps |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36. |
Heart trouble or heart murmur |
|
|
|
|
62. |
Recent gain or loss of weight |
|
|
80. Had a change in menstrual pattern |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. |
High blood pressure |
|
|
|
|
|
|
63. |
Excessive bleeding or easy bruising |
|
|
81. Are you now pregnant? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38. |
Coughed up or vomited blood |
|
|
|
|
64. |
Tumor, growth, cyst, or cancer |
|
|
82. Date of last menstrual period (YYYYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
39. |
Stomach, liver, or intestinal trouble |
|
|
65. |
Considered or attempted suicide |
|
|
|
|
|
|
|
|
DD FORM 2492, MAR 2008 |
|
|
PREVIOUS EDITION IS OBSOLETE. |
DoD Exception to SF93 approved by GSA/IRMS (8-91) |