
With the help of the online PDF tool by FormsPal, you're able to complete or edit Dd Form 2792 1 here. Our team is aimed at providing you with the perfect experience with our editor by consistently adding new functions and improvements. With these improvements, using our tool becomes better than ever! To begin your journey, consider these easy steps:
Step 1: Hit the orange "Get Form" button above. It is going to open up our pdf tool so that you can begin filling in your form.
Step 2: With this state-of-the-art PDF tool, you can accomplish more than merely fill out blank fields. Edit away and make your documents appear faultless with customized textual content added in, or optimize the file's original input to perfection - all that comes with an ability to add your personal graphics and sign the document off.
For you to finalize this PDF document, ensure you type in the information you need in each field:
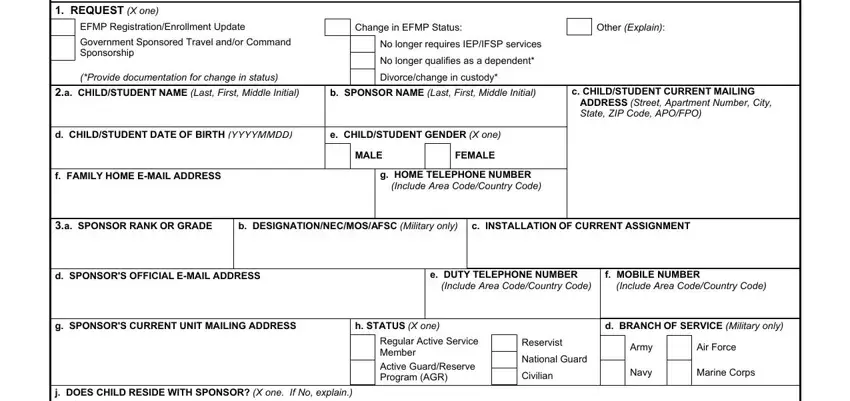
1. Fill out the Dd Form 2792 1 with a selection of necessary fields. Gather all of the important information and make certain there is nothing forgotten!
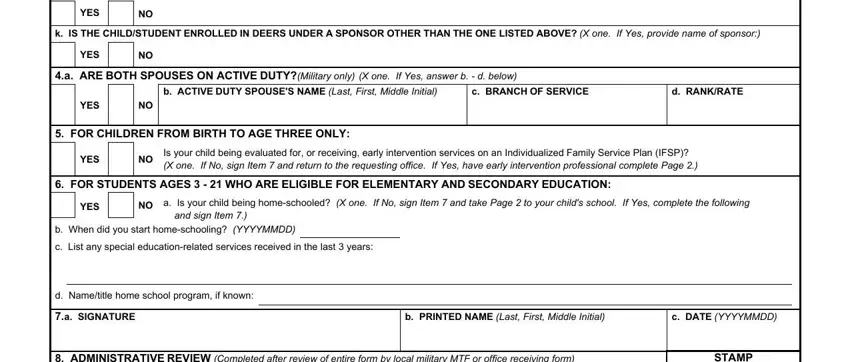
2. Just after this array of fields is filled out, go to enter the relevant information in all these - YES, k IS THE CHILDSTUDENT ENROLLED IN, YES, a ARE BOTH SPOUSES ON ACTIVE, b ACTIVE DUTY SPOUSES NAME Last, c BRANCH OF SERVICE, d RANKRATE, YES, FOR CHILDREN FROM BIRTH TO AGE, YES, Is your child being evaluated for, FOR STUDENTS AGES WHO ARE, YES, a Is your child being homeschooled, and b When did you start homeschooling.
3. In this particular stage, examine ADMINISTRATIVE REVIEW Completed, STAMP, a SPONSOR SSN, b SPOUSE SSN If dual military, c SSN USED IN DEERS If different, d FAMILY MEMBER PREFIX, e MILITARY MTF OR OFFICE RECEIVING, f DATE YYYYMMDD, DD FORM APR, and Page of Pages. All of these need to be filled in with greatest awareness of detail.

4. The subsequent part requires your input in the subsequent places: a SIGNATURE OF SPONSOR SPOUSE OR, b PRINTED NAME, c RELATIONSHIP TO CHILD STUDENT, d DATE YYYYMMDD, CHILDSTUDENT INFORMATION To be, a NAME OF CHILDSTUDENT Last First, b CURRENT GRADE LEVEL If school age, c DATE OF BIRTH YYYYMMDD, d GENDER X one, FEMALE, MALE, EARLY INTERVENTION EI SERVICES, a Is the child currently being, b Does this child receive early, and If Yes please attach current IFSP. Make certain to type in all of the requested info to go onward.
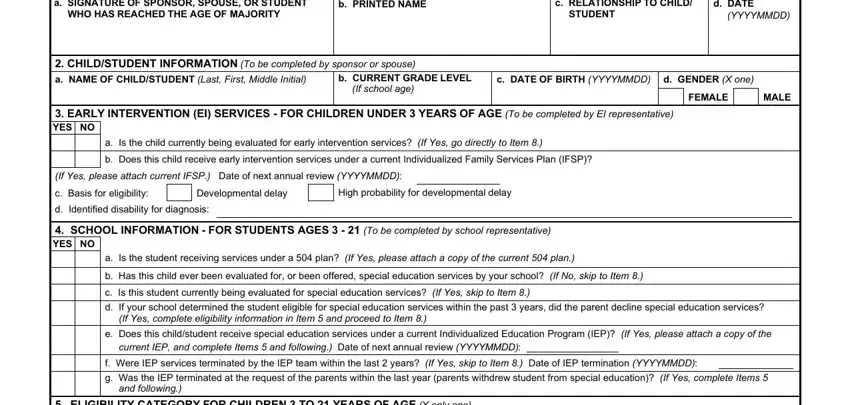
Be really mindful while filling out c DATE OF BIRTH YYYYMMDD and c RELATIONSHIP TO CHILD STUDENT, because this is where most people make errors.
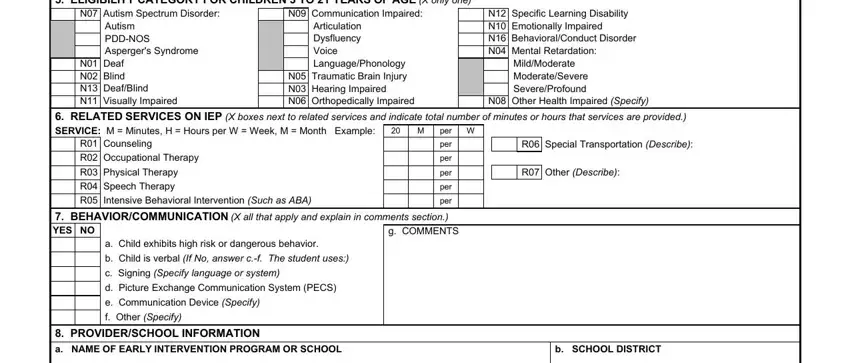
5. This very last point to complete this PDF form is pivotal. Make certain you fill in the appropriate blanks, which includes ELIGIBILITY CATEGORY FOR CHILDREN, N Autism Spectrum Disorder, N Communication Impaired, Autism PDDNOS Aspergers Syndrome, N Deaf N Blind N DeafBlind N, Articulation Dysfluency Voice, N Specific Learning Disability N, MildModerate ModerateSevere, N Other Health Impaired Specify, RELATED SERVICES ON IEP X boxes, per W, R Special Transportation Describe, R Other Describe, R Counseling, and R Occupational Therapy, prior to finalizing. Neglecting to do this could result in an unfinished and potentially incorrect document!
Step 3: Right after double-checking the filled out blanks, press "Done" and you're good to go! Join FormsPal now and immediately get Dd Form 2792 1, set for downloading. Each and every edit you make is conveniently preserved , letting you edit the pdf later on anytime. FormsPal is dedicated to the personal privacy of all our users; we ensure that all personal data going through our editor is secure.