
You could fill out dd form 2808 updated 2019 instantly with our online tool for PDF editing. The editor is constantly upgraded by our staff, receiving cool features and becoming better. To get the process started, go through these easy steps:
Step 1: Open the form inside our tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: The editor will let you modify nearly all PDF files in a range of ways. Transform it by writing any text, correct what's originally in the file, and include a signature - all within the reach of a couple of clicks!
This PDF form requires some specific details; in order to ensure accuracy and reliability, you should heed the subsequent suggestions:
1. It is important to fill out the dd form 2808 updated 2019 correctly, so be mindful while working with the parts containing these particular fields:
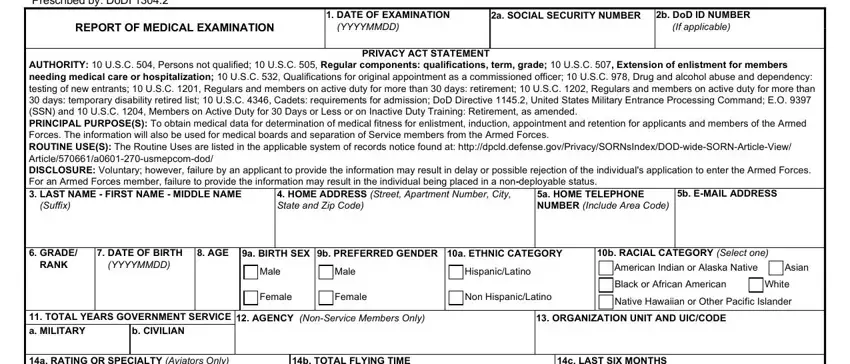
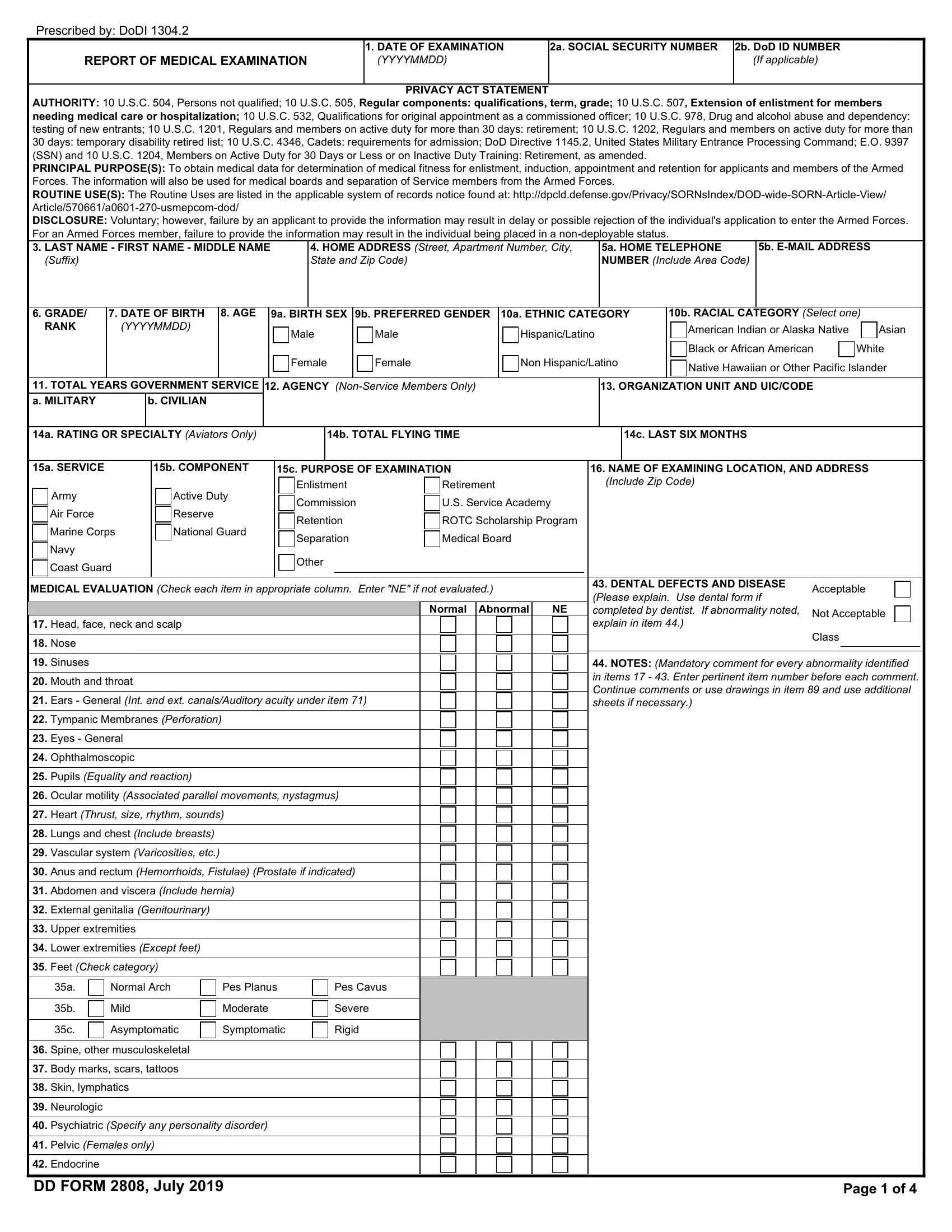
2. After the last part is complete, you have to add the needed particulars in a RATING OR SPECIALTY Aviators Only, b TOTAL FLYING TIME, c LAST SIX MONTHS, a SERVICE, b COMPONENT, c PURPOSE OF EXAMINATION, Army Air Force Marine Corps Navy, Active Duty Reserve National Guard, Enlistment Commission Retention, Other, Retirement US Service Academy ROTC, MEDICAL EVALUATION Check each item, Normal Abnormal, Head face neck and scalp Nose, and NAME OF EXAMINING LOCATION AND allowing you to go further.
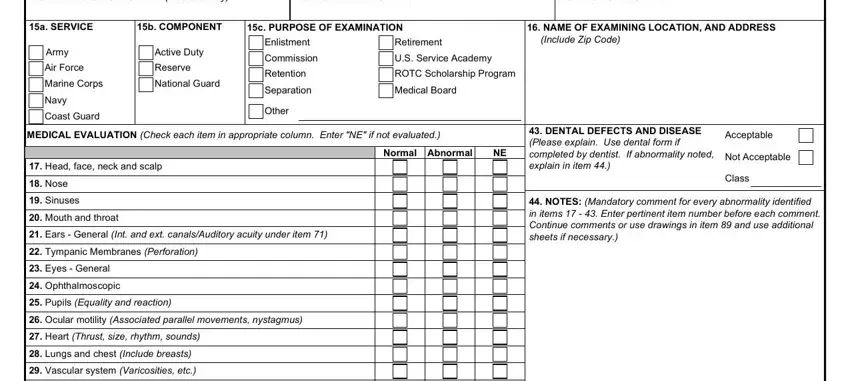
3. Completing Head face neck and scalp Nose, Normal Arch Mild Asymptomatic, Pes Planus Moderate Symptomatic, Pes Cavus Severe Rigid, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Filling out Prescribed by DoDI LAST NAME, SOCIAL SECURITY NUMBER, DoD ID NUMBER, URINALYSIS, a Albumin, b Sugar, LABORATORY FINDINGS URINE HCG, BLOOD TYPE, TESTS, RESULTS, HIV SPECIMEN ID LABEL, DRUG TEST SPECIMEN ID LABEL, HIV DRUGS ALCOHOL OTHER a PAP, HEIGHT in, and WEIGHT lbs is key in this next part - make sure you take your time and fill in each and every empty field!
5. To conclude your document, the particular section incorporates some additional blanks. Entering BLOOD PRESSURE a ST, SYS, DIAS, DISTANCE VISION Right Uncorr, b ND, SYS, DIAS, c RD, SYS, DIAS, REFRACTION, AUTO, MANIFEST, CYCLO, and Corr to will finalize the process and you'll be done in an instant!
People frequently make mistakes while filling in DIAS in this part. Be sure you read again what you type in here.
Step 3: Check all the information you have entered into the blank fields and then click on the "Done" button. After creating afree trial account with us, you will be able to download dd form 2808 updated 2019 or send it via email promptly. The PDF form will also be readily accessible via your personal account with all of your changes. FormsPal guarantees your information confidentiality by using a protected system that in no way saves or shares any type of personal data involved. Rest assured knowing your documents are kept confidential when you work with our editor!