PRIVACY ACT STATEMENT
AUTHORITY: Executive Order 9397, 10 U.S.C. Sections 1477 and 2771, P.L. 92-425 (September 21, 1972, as amended.
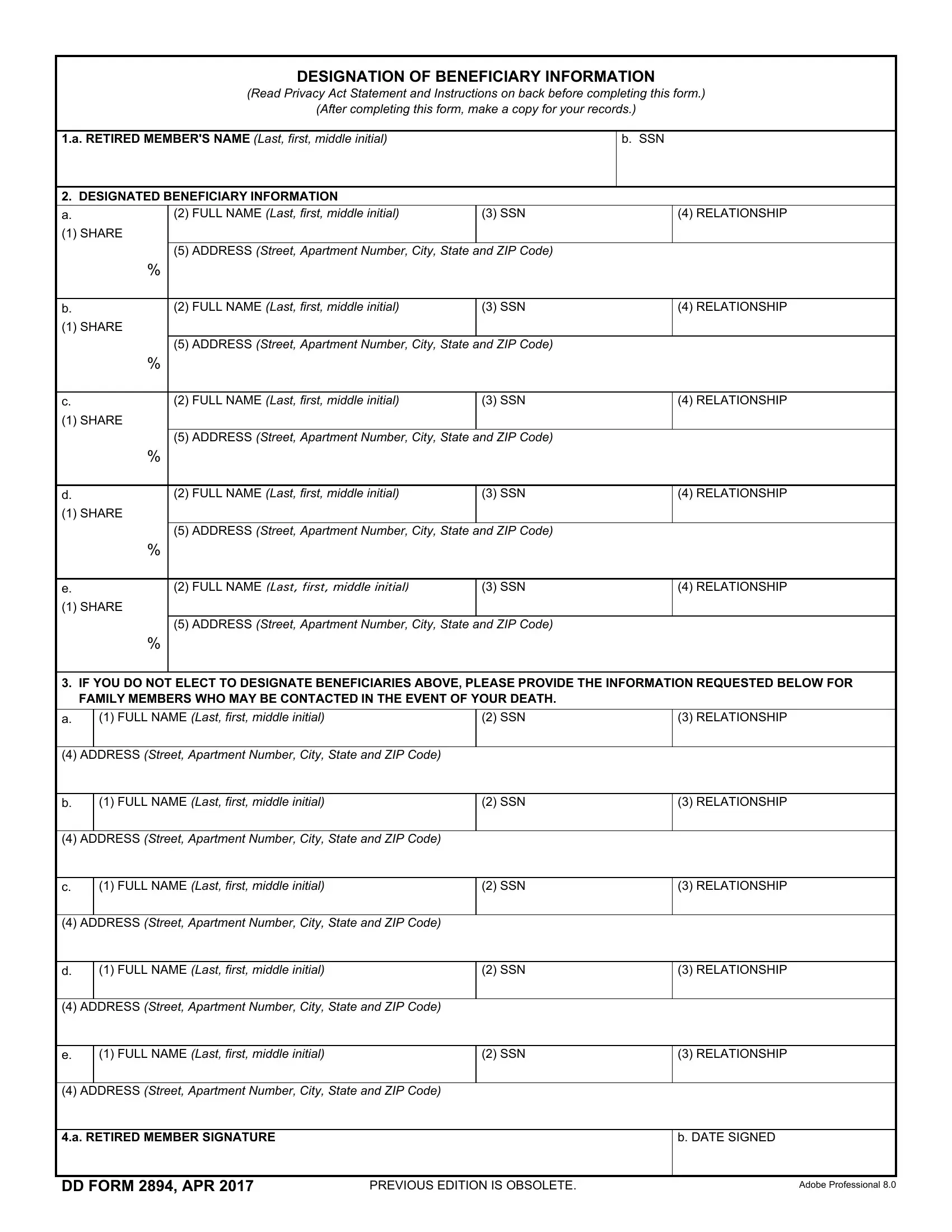
PRINCIPAL PURPOSE(S): The purpose in collecting this information is so that the retiree can designate a beneficiary to receive any retired pay still owed to that member upon his or her death.
ROUTINE USE(S): The information on this form may be disclosed as generally permitted under 5 U.S.C. Section 552(a)(b) of the Privacy Act of 1974, as amended. It may also be disclosed outside of the Department of Defense to the Internal Revenue Service for tax purposes, the Department of Veterans Affairs (DVA) for discontinuing DVA compensation, or individuals authorized to receive retired pay on behalf of the retiree. In addition, other Federal, State, or local government agencies, which have identified a need to know, may obtain this information for the purpose(s) identified in the DoD Blanket Routine Uses as published in the Federal Register.
DISCLOSURE: Disclosure is voluntary; however, failure to furnish the requested information will result in delays in payment of arrears of retirement pay, and will result in the inability to pay the designated beneficiary.
INSTRUCTIONS
This form is intended to apply to any amounts you are due as a retired member on the date of your death, including retired pay and, if you are eligible, Combat-Related Special Compensation (CRSC). References to unpaid retired pay in this form include CRSC, if applicable. Entitlement to retired pay stops on the date of your death. CRSC payments terminate on the first day of the month in which you die. In order to determine who should receive any retired pay or CRSC you are owed when you die, this form should be completed and returned to:
Defense Finance and Accounting Service
U.S. Military Retirement Pay
P.O. Box 7130
London, KY 40742-7130
By law, you may designate a beneficiary or beneficiaries you wish to receive your unpaid retired pay. If you specifically elect to designate a beneficiary or beneficiaries, you must list the names of the beneficiaries you desire in the top part of the form (Item 2), their relationship to you (Item 4), their SSN (if available) (Item 3), and their address (Item 5). You can either provide a SHARE percentage to be paid to each person or leave the SHARE percentage blank. If you leave the SHARE percentage blank, any retired pay you are owed when you die will be divided equally among your designated beneficiaries. Complete all other requested information. If you list more than one person with a 100% SHARE, we will pay in the order of the beneficiaries as you list them on the form. If, for example, you designate two beneficiaries, then the SHARE percentage can be blank, 100% for each beneficiary, or the SHARE percentages when added together must equal 100%. Similarly, if you designate three beneficiaries, then the SHARE percentage can be blank or equal one of the following combinations: 100% for each of the beneficiaries; or, if you designate 100% for one of the beneficiaries, the sum of the SHARE percentage for the remaining two must equal 100%; or, the sum of the SHARE percentage for all three beneficiaries must be 1/3 each. If you designate beneficiaries, you should update your beneficiary information whenever there is a change in your marital status or whenever you choose different beneficiaries.
If you designate more than 5 beneficiaries, you must submit your beneficiary designation in a signed letter to the return address listed above. To be valid, a beneficiary designation must be received by DFAS before the date of your death.
If you are not specifically designating beneficiaries, complete the bottom of the form (Item 3) with the Name, Social Security Number (if available), Relationship and Address of your living family members who may be contacted upon your death regarding the unpaid retired pay. The names provided should include spouse, children, parents and siblings. If you do not elect to specifically designate beneficiaries to receive your unpaid retired pay upon your death, or the designated beneficiary dies before you, the amount due will be paid to the person or person(s) highest on the following list living at the time of your death: (1) your spouse; (2) your children and their descendants, by representation; (3) your parents, in equal parts, or if either is dead, the survivor; (4) the legal representative of your estate; and (5) persons entitled under the law of your domicile. When you complete the form, you must enter your Social Security Number and sign the form. Forms or letters that contain incorrect SHARE percentages will be returned for correction. Forms or letters that do not contain your Social Security Number or your signature will be returned to you unprocessed.