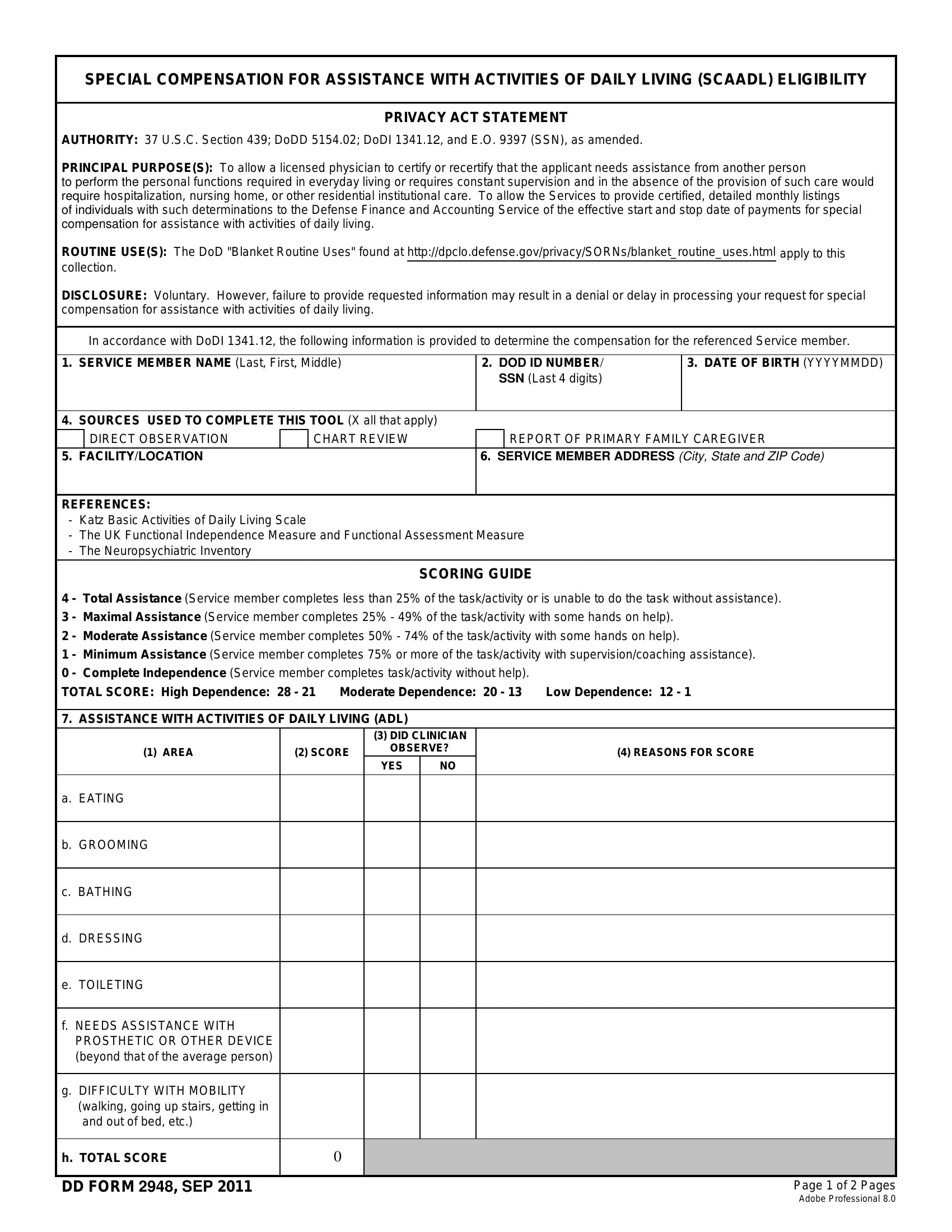
At the heart of providing care for those who have sacrificed for their nation lies the DD Form 2948, a document specifically designed to assess and determine the level of Special Compensation for Assistance with Activities of Daily Living (SCAADL) for eligible service members. This important form is guided by authoritative legislation and directives, including 37 U.S.C. Section 439, DoDD 5154.02, and DoDI 1341.12, ensuring that the process adheres to a structured and legal framework. The principal purpose of the DD Form 2948 is multifaceted: it allows a licensed physician to certify the need for assistance in daily living due to a service member's inability to perform personal functions or the requirement for constant supervision. Additionally, it outlines a system for calculating the compensation through a detailed scoring guide based on the Katz Basic Activities of Daily Living Scale, among other references. This assessment covers eating, grooming, bathing, mobility, and the need for supervision for safety reasons, providing a comprehensive look at the individual's requirements for assistance. With its intricate design, the form serves not only as a tool for assessment but also communicates the Defense Finance and Accounting Service's (DFAS) role in processing the compensation. It underscores the gravity of disclosing necessary information — a step that is voluntary, yet essential for rendering aid to those in need. Ultimately, the DD Form 2948 embodies a critical process in acknowledging and supporting the profound needs of service members requiring assistance in their daily lives.
| Question | Answer |
|---|---|
| Form Name | Dd Form 2948 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dd 2948, ICD-09, ADL, Katz |
SPECIAL COMPENSATION FOR ASSISTANCE WITH ACTIVITIES OF DAILY LIVING (SCAADL) ELIGIBILITY
PRIVACY ACT STATEMENT
AUTHORITY: 37 U.S.C. Section 439; DoDD 5154.02; DoDI 1341.12, and E.O. 9397 (SSN), as amended.
PRINCIPAL PURPOSE(S): To allow a licensed physician to certify or recertify that the applicant needs assistance from another person
to perform the personal functions required in everyday living or requires constant supervision and in the absence of the provision of such care would require hospitalization, nursing home, or other residential institutional care. To allow the Services to provide certified, detailed monthly listings
of individuals with such determinations to the Defense Finance and Accounting Service of the effective start and stop date of payments for special compensation for assistance with activities of daily living.
ROUTINE USE(S): The DoD "Blanket Routine Uses" found at http://dpclo.defense.gov/privacy/SORNs/blanket_routine_uses.html apply to this collection.
DISCLOSURE: Voluntary. However, failure to provide requested information may result in a denial or delay in processing your request for special compensation for assistance with activities of daily living.
In accordance with DoDI 1341.12, the following information is provided to determine the compensation for the referenced Service member.
1.SERVICE MEMBER NAME (Last, First, Middle)
2.DOD ID NUMBER/ SSN (Last 4 digits)
3. DATE OF BIRTH (YYYYMMDD)
4. SOURCES USED TO COMPLETE THIS TOOL (X all that apply)
|
DIRECT OBSERVATION |
|
CHART REVIEW |
|
REPORT OF PRIMARY FAMILY CAREGIVER |
5. FACILITY/LOCATION |
|
|
6. SERVICE MEMBER ADDRESS (City, State and ZIP Code) |
||
|
|
|
|
|
|
REFERENCES:
-Katz Basic Activities of Daily Living Scale
-The UK Functional Independence Measure and Functional Assessment Measure
-The Neuropsychiatric Inventory
|
|
SCORING GUIDE |
|
4 |
- Total Assistance (Service member completes less than 25% of the task/activity or is unable to do the task without assistance). |
||
3 |
- Maximal Assistance (Service member completes 25% - 49% of the task/activity with some hands on help). |
||
2 |
- Moderate Assistance (Service member completes 50% - 74% of the task/activity with some hands on help). |
||
1 |
- Minimum Assistance (Service member completes 75% or more of the task/activity with supervision/coaching assistance). |
||
0 |
- Complete Independence (Service member completes task/activity without help). |
|
|
TOTAL SCORE: High Dependence: 28 - 21 |
Moderate Dependence: 20 - 13 |
Low Dependence: 12 - 1 |
|
7.ASSISTANCE WITH ACTIVITIES OF DAILY LIVING (ADL)
(3)DID CLINICIAN
(1) AREA |
(2) SCORE |
OBSERVE? |
(4) REASONS FOR SCORE |
|
|
|
YES |
NO |
|
|
|
|
|
|
a.EATING
b.GROOMING
c.BATHING
d.DRESSING
e.TOILETING
f.NEEDS ASSISTANCE WITH PROSTHETIC OR OTHER DEVICE (beyond that of the average person)
g.DIFFICULTY WITH MOBILITY (walking, going up stairs, getting in and out of bed, etc.)
h. TOTAL SCORE |
0 |
|
|
|
|
DD FORM 2948, SEP 2011 |
|
Page 1 of 2 Pages |
Adobe Professional 8.0
8. |
SUPERVISION/PROTECTION (Use Scoring Guide on Page 1) |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(3) DID CLINICIAN |
|
|
|
|
|||
|
(1) AREA |
(2) SCORE |
OBSERVE? |
|
|
(4) REASONS FOR SCORE |
||||
|
|
|
|
|
|
|
||||
|
|
|
YES |
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. REQUIRES SUPERVISION/ |
|
|
|
|
|
|
|
|
|
|
|
ASSISTANCE AS A RESULT OF |
|
|
|
|
|
|
|
|
|
|
SEIZURES (blackouts or lapses in |
|
|
|
|
|
|
|
|
|
|
mental awareness, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. DIFFICULTY WITH PLANNING |
|
|
|
|
|
|
|
|
|
|
|
AND ORGANIZING (able to adhere |
|
|
|
|
|
|
|
|
|
|
to medication regimen, managing |
|
|
|
|
|
|
|
|
|
|
financial and other household |
|
|
|
|
|
|
|
|
|
|
affairs, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. SAFETY RISKS (significant risk of |
|
|
|
|
|
|
|
|
|
|
|
falling, wandering outside the |
|
|
|
|
|
|
|
|
|
|
home, leaving cook top/oven on, |
|
|
|
|
|
|
|
|
|
|
crossing streets, using electrical |
|
|
|
|
|
|
|
|
|
|
appliances, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. DIFFICULTY WITH SLEEP |
|
|
|
|
|
|
|
|
|
|
|
REGULATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. REQUIRES ASSISTANCE/ |
|
|
|
|
|
|
|
|
|
|
|
SUPERVISION AS A RESULT OF |
|
|
|
|
|
|
|
|
|
|
DELUSIONS/HALLUCINATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f. DIFFICULTY WITH RECENT |
|
|
|
|
|
|
|
|
|
|
|
MEMORY (forgets what day it is, |
|
|
|
|
|
|
|
|
|
|
what happened yesterday, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
g. SELF REGULATION (being able to |
|
|
|
|
|
|
|
|
|
|
|
moderate moods, agitation/ |
|
|
|
|
|
|
|
|
|
|
aggression) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H. TOTAL SCORE |
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. TOTAL SCORES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
a. ADL |
b. SUPERVISION/PROTECTION |
c. TOTAL |
|
d. DEPENDENCE LEVEL |
||||||
|
0 |
|
0 |
|
|
|
|
|
0 |
|
|
|
|
|
|
|
|
|
|
|
|
10. APPLICABLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
11.A PERSON COMPLETING FORM (Name and Signature) |
|
|
|
|
|
b. DATE |
||||
|
|
|
|
|
|
|
|
|||
c. PRINTED NAME OF PHYSICIAN (Last, First, Middle Initial) |
|
|
d. TITLE |
|
|
|||||
|
|
|
|
|
|
|
|
|||
e. TELEPHONE (Include area code) |
f. EMAIL ADDRESS |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
12. SERVICE MEMBER ACKNOWLEDGEMENT |
|
|
|
|
|
|
|
|
||
|
I acknowledge my PCM's assessment of my dependency level. I |
|
do |
|
do not plan to appeal this decision. |
|||||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|||
a. PERSON COMPLETING FORM (Name and Signature) |
|
|
|
|
|
b. DATE |
||||
|
|
|
|
|
|
|
|
|||
c. TELEPHONE (Include area code) |
d. EMAIL ADDRESS |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
DD FORM 2948, SEP 2011 |
Page 2 of 2 Pages |