
When working in the online PDF tool by FormsPal, you can complete or change 2008 here. To make our editor better and less complicated to use, we consistently design new features, taking into account suggestions coming from our users. In case you are seeking to start, here is what it will take:
Step 1: Firstly, access the pdf tool by pressing the "Get Form Button" above on this site.
Step 2: This tool enables you to work with almost all PDF forms in a range of ways. Enhance it by adding your own text, correct what is already in the document, and add a signature - all within a few mouse clicks!
Pay close attention when completing this pdf. Ensure all mandatory blank fields are filled in properly.
1. When filling in the 2008, be certain to complete all of the important blanks in the relevant section. It will help speed up the process, allowing for your information to be handled without delay and accurately.
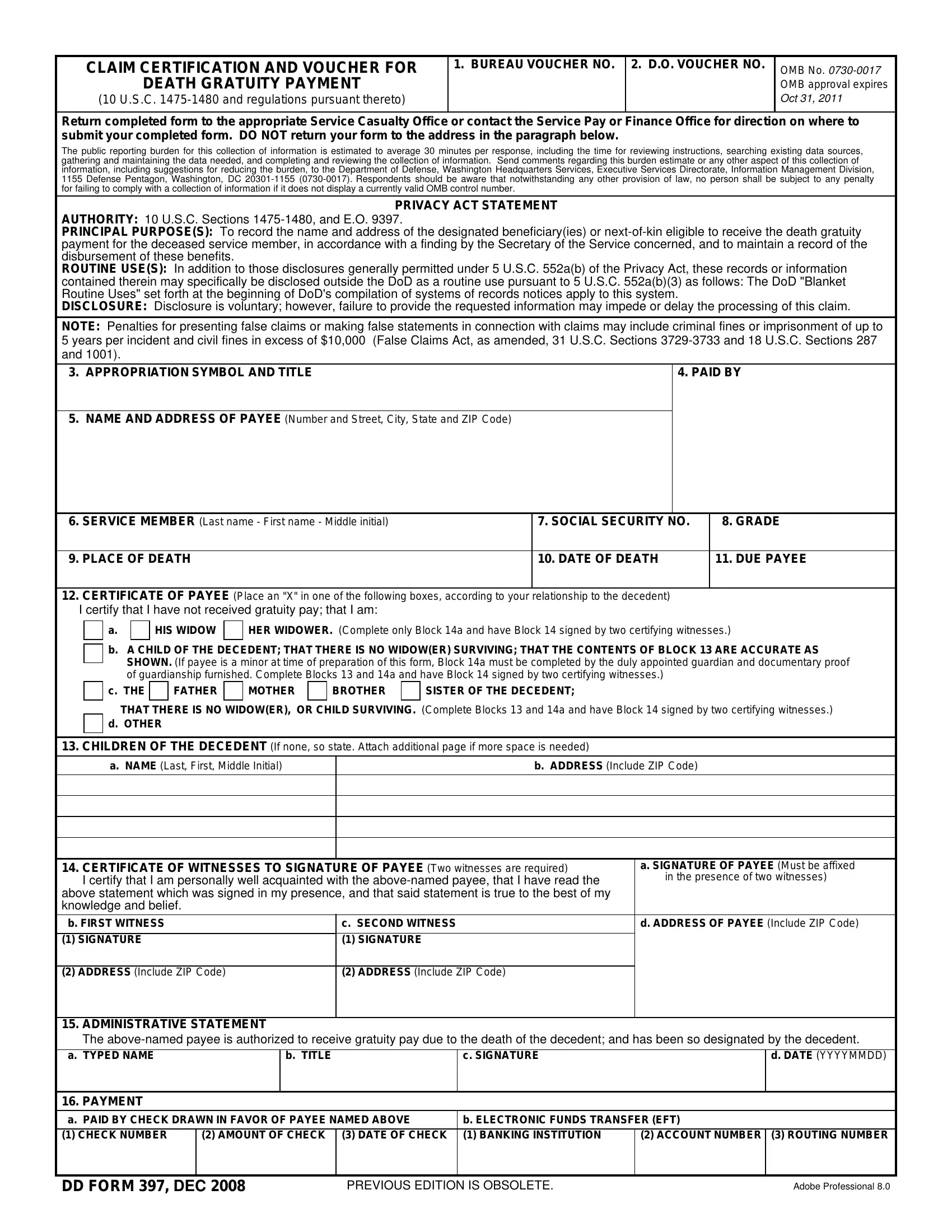
2. Right after completing the previous step, head on to the next part and fill out all required particulars in these blank fields - CERTIFICATE OF PAYEE Place an X, HIS WIDOW, HER WIDOWER Complete only Block a, b A CHILD OF THE DECEDENT THAT, SISTER OF THE DECEDENT, BROTHER, MOTHER, FATHER, CHILDREN OF THE DECEDENT If none, a NAME Last First Middle Initial, b ADDRESS Include ZIP Code, CERTIFICATE OF WITNESSES TO, c SECOND WITNESS SIGNATURE, a SIGNATURE OF PAYEE Must be, and d ADDRESS OF PAYEE Include ZIP Code.

As to a SIGNATURE OF PAYEE Must be and BROTHER, make sure you don't make any errors in this current part. The two of these are viewed as the most significant fields in the file.
3. Completing ADMINISTRATIVE STATEMENT The, c SIGNATURE, b TITLE, d DATE YYYYMMDD, PAYMENT a PAID BY CHECK DRAWN IN, AMOUNT OF CHECK, DATE OF CHECK, b ELECTRONIC FUNDS TRANSFER EFT, ACCOUNT NUMBER ROUTING NUMBER, DD FORM DEC, PREVIOUS EDITION IS OBSOLETE, and Adobe Professional is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: After you have glanced through the details in the file's blank fields, click on "Done" to complete your document generation. Make a 7-day free trial subscription with us and get immediate access to 2008 - download or modify from your FormsPal cabinet. We don't sell or share the information that you use while completing forms at our site.