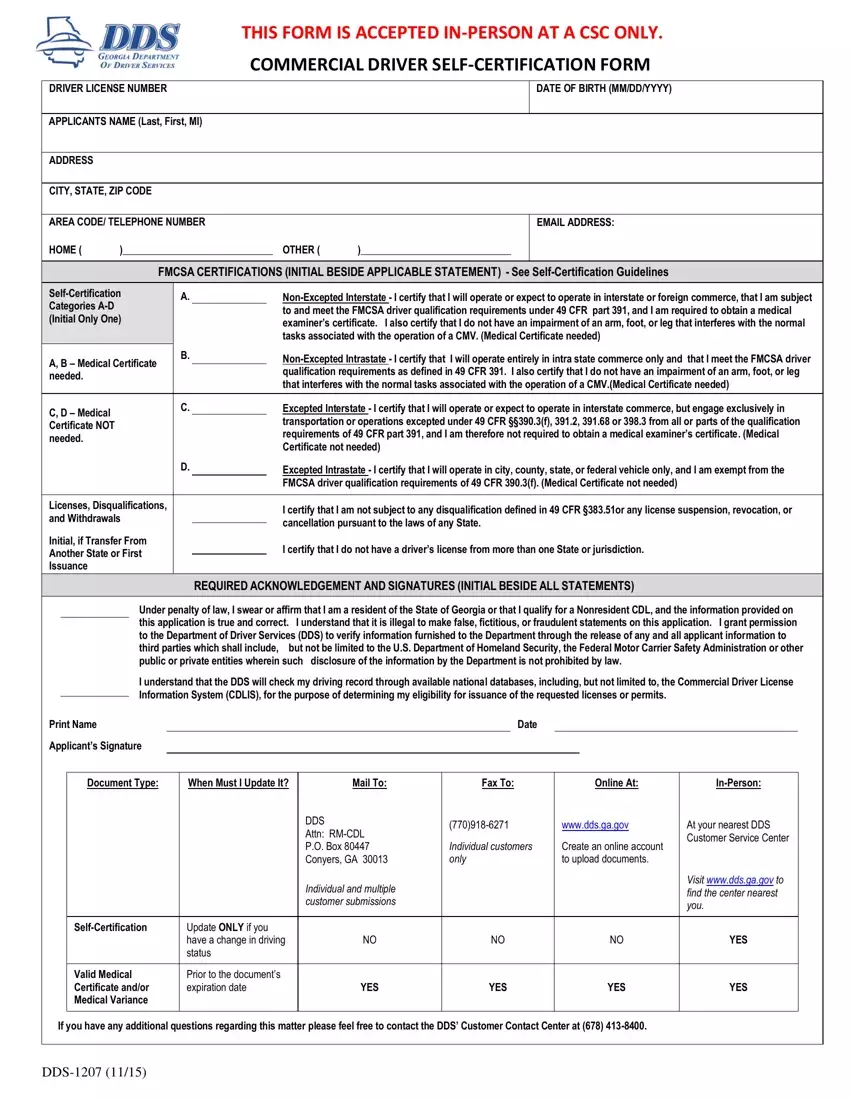
Understanding the DDS 1207 form is vital for commercial drivers operating within the State of Georgia. This Commercial Driver Self-Certification Form plays a crucial role in ensuring that drivers meet the Federal Motor Carrier Safety Administration (FMCSA) regulations, particularly regarding medical fitness for duty. By filling out this form, drivers provide critical information including their license number, date of birth, contact details, and make specific certifications about the nature of their commercial driving activities—whether operating interstate or intrastate, and if their operations are excepted or non-excepted from FMCSA's medical certification requirements. Additionally, the form requires drivers to certify that they are not subject to any disqualifications, license suspensions, revocations, or cancellations, and that they hold a valid driver’s license from only one state. It emphasizes honesty and accuracy by requiring a signed acknowledgment under penalty of law, ensuring that all provided information is true. The process outlined for submitting the DDS 1207 includes various options such as mail, fax, online, or in-person submissions, clearly designed to accommodate the needs of individual drivers and streamline the self-certification process. This introduction invites commercial drivers and stakeholders within the transportation industry to appreciate the significance of the DDS 1207 form in promoting road safety and compliance with federal and state regulations.
| Question | Answer |
|---|---|
| Form Name | Dds 1207 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cdl medical self certification form, self certification, dds self certification form, form 1207 |
