DDS Mail-in Renewal Options
Thank you for your interest in renewing your Georgia driver’s license, permit, or ID card. The Georgia Department of Driver Services offers renewal by mail options under limited circumstances for U.S. citizen customers who are unable to renew their license in person.
The following customers may utilize this option:
Customers stationed out of state in the military, and their dependents stationed with them
Customers attending school out of the State of Georgia, and their dependents who are with them
Customers temporarily working out of state, and their dependents who are with them
Customers who are physically incapacitated and unable to visit a DDS Customer Service Center
The following general requirements and conditions apply:
You must be a U.S. Citizen.
If you are changing your Georgia address as part of your renewal, you must include proof of the new address. A listing of acceptable documents for this purpose is enclosed.
The customer requesting renewal must complete the DDS-23S form (Application for Driver’s License, Permit, or Identification Card) and have it notarized in Section F.
Customers 60 years of age or older must provide verification that vision requirements are met if applying to renew a driver’s license or permit (enclosed Vision Form must be completed).
Only a 5-year renewal is allowed through this method. 8-year renewal is not allowed by mail.
The customer must provide payment of $20 for a 5-year renewal, payable by check, money order, or credit card.
Processing can take up to ten business days from receipt of your application package. Failure to provide all required documents will delay renewal of your license. Expedited processing is not available. Requests will be processed on a first-come, first-serve basis.
Only renewal of non-commercial licenses, permits, and ID’s is available by mail. Renewal of Commercial Driver’s Licenses (CDL’s) must be done in person at a DDS location.
To complete renewal by mail, please mail all required documents (see reverse side for specific requirements) to the following address along with your payment:
DDS Special Issuance
2206 Eastview Parkway
Conyers, GA 30013
Please make checks or money orders payable to DDS for the renewal fee of $20. A separate check or money order is required for each customer’s renewal request. If paying by credit card, please complete the enclosed Credit Card Authorization Form and return with your application package.
The chart on the back of this page lists the documents required for each type of renewal. Blank application form (DDS-23S), Vision Screening Results form if applicable (DDS-274A), and Credit Card Authorization (DDS-100) form are enclosed for completion.
Please direct any questions to our Customer Contact Center at 1-866-754-3687.
DDS Mail-in Renewal Requirements
Please check the section that applies to you and submit all required documents in that section.
Include this form with your documents.
Note: 8-year renewal is not available by mail.
|
Military |
|
Students |
1. |
DDS-23S application completed and notarized |
1. |
DDS-23S application completed and notarized |
2. |
Vision Screening Results Form (DDS-274A) |
2. |
Vision Screening Results Form (DDS-274A) |
|
completed (if applicable) |
|
completed (if applicable) |
3. |
Payment of $20 (check, money order, or credit |
3. |
Payment of $20 (check, money order, or credit |
|
card authorization) |
|
card authorization) |
4. |
Signed letter from Commanding Officer on |
4. |
Signed letter from an official at the school on |
|
military unit letterhead verifying that the |
|
school letterhead verifying that the student |
|
customer (referenced by name) is currently |
|
(referenced by name) is currently enrolled in |
|
serving at the location, or that the customer |
|
the school, or that the customer (referenced by |
|
(referenced by name) is the spouse or |
|
name) is the spouse or dependent of a student |
|
dependent of a member of the military |
|
(referenced by name) currently enrolled in the |
|
(referenced by name) currently serving at the |
|
school |
|
location |
|
|
|
Temporarily Employed Out of State |
|
Physically Unable to Visit CSC in Person |
1. |
DDS-23S application completed and notarized |
1. |
DDS-23S application completed and notarized |
2. |
Vision Screening Results Form (DDS-274A) |
2. |
Vision Screening Results Form (DDS-274A) |
|
completed (if applicable) |
|
completed (if applicable) |
3. |
Payment of $20 (check, money order, or credit |
3. |
Payment of $20 (check, money order, or credit |
|
card authorization) |
|
card authorization) |
4. |
Signed letter from the customer’s employer on |
4. |
Signed verification from a licensed physician |
|
employer letterhead verifying that the customer |
|
that the customer is incapacitated and unable to |
|
(referenced by name) is temporarily employed |
|
visit a DDS Customer Service Center in person |
|
outside the State of Georgia, or that the |
|
to renew |
|
customer (referenced by name) is the spouse or |
|
|
|
dependent of an employee (referenced by |
|
|
|
name) temporarily employed outside the State |
|
|
|
of Georgia |
|
|
Please mail all required documents to the following address along with your payment of $20 (no fee if customer holds a current Veteran license):
DDS Special Issuance
2206 Eastview Parkway
Conyers, GA 30013
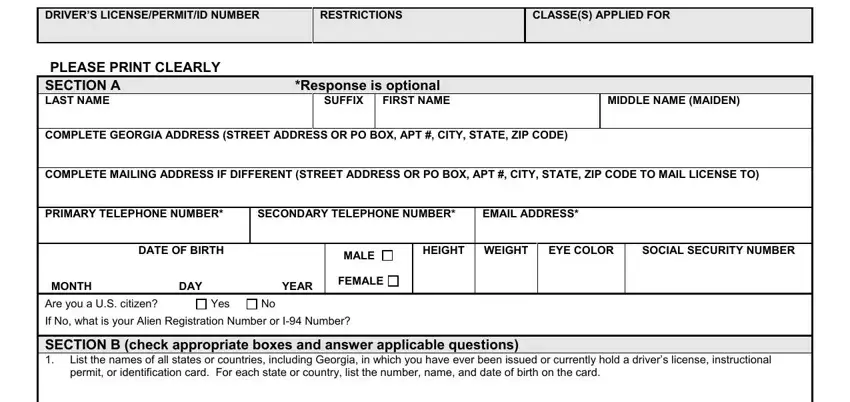
APPLICATION FOR DRIVER’S LICENSE, PERMIT,
OR IDENTIFICATION CARD
DRIVER’S LICENSE/PERMIT/ID NUMBER
PLEASE PRINT CLEARLY
|
SECTION A |
|
*Response is optional |
|
|
|
|
|
|
LAST NAME |
|
|
|
SUFFIX |
FIRST NAME |
|
|
MIDDLE NAME (MAIDEN) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE GEORGIA ADDRESS (STREET ADDRESS OR PO BOX, APT #, CITY, STATE, ZIP CODE) |
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE MAILING ADDRESS IF DIFFERENT (STREET ADDRESS OR PO BOX, APT #, CITY, STATE, ZIP CODE TO MAIL LICENSE TO) |
|
|
|
|
|
|
|
|
|
|
|
PRIMARY TELEPHONE NUMBER* |
SECONDARY TELEPHONE NUMBER* |
EMAIL ADDRESS* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
MALE |
HEIGHT |
WEIGHT |
EYE COLOR |
SOCIAL SECURITY NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FEMALE |
|
|
|
|
|
|
|
MONTH |
DAY |
YEAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If No, what is your Alien Registration Number or I-94 Number?
SECTION B (check appropriate boxes and answer applicable questions)
1.List the names of all states or countries, including Georgia, in which you have ever been issued or currently hold a driver’s license, instructional permit, or identification card. For each state or country, list the number, name, and date of birth on the card.
2.List the names of all states or countries, including Georgia, in which your driver’s license, instructional permit, or identification card, or privilege to drive is currently revoked, suspended, canceled, or denied. For each state or country, list the reason and when the action was taken.
3.Is your driver’s license being held by a police officer, law enforcement agency, or court in this state or any other
state or country? |
If Yes, explain: |
If applying for a driver’s license or instructional permit, do you wear glasses or contact lenses for driving?
Vision Screening Results Field of Vision |
With Lenses |
Without Lenses |
FOR DEPARTMENTAL USE ONLY
DO NOT WRITE IN THIS SPACE
|
|
|
|
|
|
|
Sight Screener |
Right |
|
20/ |
20/ |
Doctor Certificate |
Left |
|
20/ |
20/ |
Bioptics |
Both |
|
|
20/ |
20/ |
5. |
Are you a habitual user of alcohol or any drug to a degree which renders you incapable of safely driving a motor vehicle? |
Yes |
No |
|
|
|
|
6. |
Have you ever had seizures, fainting, heart trouble, hearing problems, musculoskeletal performance problems, or respiratory |
Yes |
No |
|
function problems? If Yes, date of last incident: ____ /____ /____ |
|
|
|
Please describe and provide physician name and city: |
|
|
7.Have you ever been diagnosed with any mental disability or disease? If yes, have ever been rendered incompetent?
If so, are you currently restored to competency by the methods provided by law?
8.Do you have any identical brother(s) or sister(s)? If Yes, list full name(s):
Yes |
No |
Yes |
No |
Yes |
No |
Yes |
No |
9. |
Do you wish to have “Organ Donor” displayed on your license or ID? |
|
Yes |
No |
|
|
|
|
|
10. |
If applying for a driver’s license or instructional permit, do you want to donate $1 for the prevention of blindness? |
N/A |
Yes |
No |
|
|
|
|
|
11. |
If you are a male U.S. citizen under the age of 26, have you registered with the Selective Service System? |
N/A |
Yes |
No |
The Georgia Department of Driver Services is required to ask all males under the age of 26 who are U.S. citizens whether they have registered with the U.S. Selective Service System, and to report the responses to the U.S. Selective Service System. Your response today does not initiate registration with the U.S. Selective Service System, however, you may be contacted by that agency as a result of your response. Your signature on this application serves as an indication that you have already registered with the U.S. Selective Service System or that you are authorizing the department to forward the necessary information to that agency for such registration. Your signature on this application constitutes consent to be registered with the U.S. Selective System if you are not already so registered. O.C.G.A. §40-5-8.
SECTION C – Lost/Stolen License
If you cannot surrender your license for any reason, please check the appropriate box below:
I am unable to surrender my SUSPENDED or REVOKED driver’s license to DDS because it is lost, or for some other reason, surrender is not possible.
I am seeking renewal or replacement of my lost Georgia driver’s license, permit, or identification card. I hereby swear or affirm that my Georgia driver’s license/permit/ID card is not currently revoked, suspended, cancelled, or denied; nor is it being held by a police officer, law enforcement agency, licensing jurisdiction, or court in this or any other state.
SECTION D – Emergency Contact Information
|
Name |
Telephone Number |
Relationship |
|
|
|
|
|
|
|
|
Relative |
Friend |
|
Other |
|
|
|
|
|
|
|
|
|
|
SECTION E – Voter Registration Application |
|
|
|
|
|
|
|
1. |
Do you want to register to vote? |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
2. |
If you are requesting a change of address on this application, is the change of address for voter registration purposes also? |
Yes |
No |
|
Your signature in this section serves as an attestation under penalty of perjury that all of the following requirements have been met:
√I am a citizen of the United States, and I am a resident of the State of Georgia and of the county or municipality in which I seek to vote.
√I am 18 years of age or older or will be 18 years of age within six months of the date of my application.
√I am not serving a sentence for having been convicted of a felony involving moral turpitude.
√I have not been judicially determined to be mentally incompetent, or if such determination has been made, the disability has been removed.
WARNING: Any person who registers to vote knowing that such person does not possess the qualifications required by law, who registers under any name other than such person’s own legal name, or who knowingly gives false information in registering, shall be guilty of a felony.
SECTION F – Required Signatures
Under penalty of law, I swear or affirm that I am a resident of the State of Georgia, and the information provided on this application is true and correct. I understand that it is illegal to make false, fictitious, or fraudulent statements on this application. I grant permission to the Department of Driver Services to verify information furnished to the Department through the release of any and all applicant information to third parties which shall include, but not be limited to the U.S. Department of Homeland Security or other public or private entities wherein such disclosure of the information by the Department is not prohibited by law.
Applicant’s Signature |
|
|
Date |
/ |
/ |
NOTARY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEAL |
Notary Signature |
|
Date |
|
/ |
/ |
|
|
The section below must be completed if applicant is under 18 years of age: |
|
|
|
|
|
|
I,
the issuance of this driver’s license or instructional permit. and that the information provided here is true and correct.
,hereby certify that I am the parent, guardian, or responsible adult approving I further certify that I have reviewed the information contained in this application,
|
|
|
|
|
|
|
|
|
Signature (Parent, Guardian, or Authorized Person) |
|
Date |
/ |
/ |
Date of Birth |
/ |
/ |
Driver’s License/Identification/Social Security Number |
|
|
|
|
FOR DEPARTMENTAL USE ONLY
Non-Commercial Exam Results
Date
Class
Law
Road Signs
Motorcycle RT
Road Test
General Observations / Retake Reason:
Georgia Department of Driver Services
Application for Non-Commercial License
Vision Screening Results
Instructions: Section A must be completed by the applicant. Sections B and C must be completed by an optometrist or ophthalmologist currently licensed to practice in the United States, and the applicant must sign the form in Section C in the presence of the optometrist or ophthalmologist.
SECTION A – CUSTOMER INFORMATION – TO BE COMPLETED BY APPLICANT
Driver’s License Number _____________________ Date of Birth ________________
Applicant’s Full Legal Name _______________________________________________
Applicant’s Complete Address _____________________________________________
______________________________________________________________________
SECTION B – VISUAL EXAMINATION RESULTS
1. Visual Acuity |
Right eye – 20/______ |
Left eye – 20/______ |
2. Horizontal Field of Vision
Right _______ Degrees |
Left _______ Degrees |
3. Were corrective lenses used for these results? Yes
Check here if correction is achieved with other than conventional lenses (bioptics). If box is checked, a detailed report must be attached.
IMPORTANT: For proper identification, please have the person whom you have examined sign the report in your presence.
SIGN HERE: ________________________________________________________
Date of examination ____________
Comments __________________________________________________________
___________________________________________________________________
___________________________________________________________________
SECTION C – OPTOMETRIST / OPTHALMOLOGIST CERTIFICATION
I __________________________________________________ being licensed to practice in
the state of ____________________, hereby certify that I have personally examined the vision
of the above named, that the results indicated on this form represent a true record of my examination and that he or she signed this form in my presence.
Printed Name of Optometrist/Ophthalmologist
Business Address
Telephone Number |
|
License # |
Signature of Optometrist / Ophthalmologist |
Today’s Date |
DDS‐274A 9/2012

Credit Card Payment Authorization Form
Instructions: To pay by credit card, please complete both sections below.
|
CREDIT CARD HOLDER INFORMATION |
|
Please check credit card type: |
|
|
|
Visa |
MasterCard |
Discover |
American Express |
Credit card number: _____________________________ |
Expiration date :__________/__________( mm/yy ) |
Exact name as it appears on the credit card: _________________________________________________________
Billing Zip Code: _________________________________ Amount to be charged: $ _____________________
Primary phone number: ______________________________ Secondary phone number: ____________________
Cardholder Signature: _______________________________________ |
Date: ___________________ |
LICENSEE/DRIVER INFORMATION
Name as it appears on Driver's License/ID: _________________________________________________________
Licensee's Drivers License / ID number: ___________________________________________________________
Birth date: ___________ /__________ /____________ (mm/dd/yyyy)
Gender (circle one): Male Female
Please send this credit/debit card payment form and supporting documents to:
Georgia Department of Driver Services
ATTN: Validation
P. O. Box 80447
Conyers, GA 30013
What type of service is this payment for?
Mail in Renewal – Georgia Address Change
Please provide one document from the list below if your request for renewal includes a change of your address in Georgia.
Utility bill issued within the last sixty (60) days;
In general a utility bill will be for a service provided to the customer that designates their residency or service address. Common examples include telephone, mobile phone, water, sewer, electricity, gas, propane, satellite, cable TV, Internet or garbage collection.
Bank statement issued within the last sixty (60) days;
A bank statement is considered a statement, printout or letter from any financial services company.
Common examples include statements for Checking or Savings accounts, Credit Card statements, credit union statements, loan payments, auto, motorcycle and RV loans.
Currently valid rental contracts and/or receipts for payments made within the last sixty (60) days for rent payments;
This includes rental agreements and leases for a home, apartment, mobile home, dorm, extended stay hotel, etc. Common examples include rental agreement or receipt, general lease agreement, student housing contract, letter from shelters, retirement or medical centers and extended stay hotel receipts.
Employer verification, including, but not limited to, one of the following:
Employer verification may be a formal statement or letter from the company stating the residency address for the employee. Letters should be on company letterhead.
Common examples include Paycheck, Paycheck stub, W-2 form from current or preceding year (these can also be used for SSN verification).
Examples that can only be used to prove residency include letters from the employer, military orders, etc.
Non-expired Georgia driver’s license, permit or identification card issued to the applicant’s parent, guardian, spouse, or child;
For minors and dependents, unexpired GA driver’s license, permit or ID card issued to parent, guardian or spouse residing in same household. For dependent parents, unexpired GA driver’s license, permit or ID card issued to a relative residing in the same household.
Health insurance statement or explanation of benefits for claim;
This includes all health related invoices or statements for service or benefits. Specific information concerning medical conditions should be covered if possible prior to scanning.
Common examples include Health/life insurance statement or invoices, Hospital, clinic, doctor, or lab bills.
State of Georgia or Federal income tax return for current or preceding calendar year;
This includes all information mailed to the customer concerning tax matters from the State of Georgia or Federal Government.
Common examples include tax statements, bills or refund checks.
Annual social security statement for current or preceding calendar year;
This can include any documentation from the Social Security Administration that includes their address. Common examples include Annual Benefit statement, Numident record, Social Security Check.
Medicare or Medicaid statement;
This can include any documentation from the State or Federal Insurance programs.
Common examples Medicare/Medicaid statements, unemployment statements, WIC or other public assistance statements or statements issued by a Federal, State or Municipality.
School record or transcript for current or preceding calendar year;
This includes documentation from all instructional institutions public and private.
Common examples include the DS1, School transcripts, student loans or report cards.
Homeowners insurance policy or bill for current or preceding calendar year;
This includes statements or invoices from insurance or mortgage companies.
Common examples include Homeowners insurance bill, statement of claim, binder or cancellation notice.
Mortgage, payment coupon, deed, or property tax bill for current or preceding calendar year. This includes documentation for household or other real property.
Common examples include household mortgage, settlement or escrow statements, property tax bills, or vehicle registration.
Additional Approved Documents
Voter Registration card; unexpired firearms license (gun permit); unexpired Merchant Marine License; I-797A; I-797C; correspondence from DDS; other documents issued by Federal/State/Municipal government